
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Transient osteoporosis of the hip during pregnancy:
Report of two clinical cases
M Ometti2; M Vitali2; E Delmastro1; O Leone1*; F Montalbano1; V Salini1
1Università Vita-Salute San Raffaele, Milano, Italy.
2Ospedale San Raffaele, Milano, Italy.
*Corresponding Author : Orlando Leone
San Raffaele University, Residency Program in Orthopedics and Traumatology, Milan, Italy.
Email: leone.orlando@yahoo.it
Received : Nov 25, 2022
Accepted : Dec 16, 2022
Published : Dec 23, 2022
Archived : www.jcimcr.org
Copyright : © Leone O (2022).
Abstract
Transient osteoporosis of the hip is a self-limiting condition that is difficult to diagnose. It affects both men and pregnant women. The purpose of this article is to show two clinical cases that underwent two different treatments. Early diagnosis can indeed avoid surgical treatment.
Citation: Marinova L, Georgiev R, Evgeniev N. Clinical observations in three clinical cases with locally advanced chordomas. What is needed for early diagnosis with improved survival?. J Clin Images Med Case Rep. 2020; 1(1): 1005.
Introduction
Transient osteoporosis of the hip (TOH) is a rare self-limitingpathology.
It is more prevalent in men but when it occurs in women, it is most often seen during the third trimester of pregnancy [1]. The exact prevalence of TOH is unknown. The etiology of THO is unknown. This pathology is characterized by demineralization of the head and neck of the femur and of the spine. It’s currently unknown why the bone demineralization happens, but hormonal change, increased calcium demand and increased load on the joints are certainly involved [3,6]. There are many hypotheses about the possible etiology of osteoporosis in current literature. It’s possible that an intermittent compression of the mother’s obturator nerve provoked by the child’s head might be responsible the disease [6,8]. Another hypothesis highlights that patient’s functional impairment could be the cause of osteopenia [6]. Other authors state that TOH is a type of reflex sympathetic dystrophy because of the similar pattern of presentation [6]. It’s possible that also a viral infection may cause TOH, because it could stimulate osteoclastic resorption and demineralization [6,9]. The etiology of osteoporosis is thought also to be implicated in vascular processes; in particular, a venous stasis might damage lumbosacral cord and cause damage to the joint, or a transient ischemic event could be responsible of cellularnecrosis [6].
Transient osteoporosis of the hipoccurs in 3 main stages [2]:
-First stage: acute onset hip pain caused by edema; determined by trauma, microfracture, or neurovascular alteration [2]
-Second stage: increased bone resorption and demineralization [2]
-Third stage: disappearance of symptomsand radiographic changes [2]
Osteoporosis usually affects a single joint causing limitations in the performance of daily activities [4]. The main symptoms are: hip pain, claudicating gait, limping, limitation of the hip range of motion. These symptoms are unspecific and do not allow a unique diagnosis of the pathology.
Magnetic Resonance Imaging (MRI) is the gold standard method to diagnose TOH [2], because is the only imaging technique which shows the bone edema of the affected joint. The pattern of enhancement with no clear border is typical, the subchondral bone appears normal in T2-weighted or contrast-enhanced T1-weighted images and irregular band of low signal intensity represent stress fractures [2]. The duration of symptoms is statistically associated with the extent of edema but the patient differs in quantity, extent of edema and in subchondral lesions [2].
If the edema expands causing vascular compression, osteoporosis can evolve and determine avascular osteonecrosis [2].
The risk of hip osteonecrosis is greater at the end of pregnancy and after delivery [5]. Regarding treatment options, various therapies were used in the past for this pathogy: oral steroids, intra articular steroids and sympathetic blocks, but with very limited efficacy [6]. Now-a-days the most effective therapy is based on drugs that suppress bone resorption or induct bone formation like Bisphosphonate, Teriparatide and Calcitonin [2]. In particular, some cases were treated with calcitonin during pregnancy with reduced recovery times [2]. In addition, the patient will need to minimize weight-bearing activities and use crutches or a wheelchair [2]. In case the pain persists, it’s possible to carry out a hip core decompression [6]. The indication for surgical treatment is debated because on one hand it reduces pain but on the other hand it exposes the patient to possible surgical complications [6]. TOH usually heals definitively in 6-12 months. A particular case of THO treated with 30 sessions of Hyperbaric Oxygen (HBO) at 2.4 ATA, lasting 2 hours each, is also described in literature [7]. The most serious problem of this pathology is that often it is diagnosed late, when the only treatment option is prosthetic joint replacement at a young age due to secondary arthritis.
Case report 1
patient is a 29 years old women presenting in the emergency room for left hip coxalgia, one month after delivering her baby. She had no relevant medical history, she referred no usual medication (before or during pregnancy), and no smoking or drinking habits, she had a silent family history. Child birth took place by caesarean section due to the non-reassuring fetal conditions with a blood loss of 1200 cc. During the hospitalization uterotonic, antibiotics, analgesic therapy, iron therapy and folic acid were administered. The physical examination showed antalgic gait left hip pain and no vascular or nervous deficit. The women referred the pain started suddenly 3 months before. Passive flexion and extension of the left hip elicited pain at extreme degrees of range of motion. Internal rotation of the left hip was painful and restricted while external rotation was complete and not painful. Other joints appeared normal. Log roll, Faber, Patrick and Fadir tests were positive. Ober test and Trendelenburg tests were negative. She performed two days earlier a MRI (Figure 1) without contrast that showed: “edema of the spongy bone in the head and neck of the left femur.” In the sub capital region, a hypointense rhyme was appreciable in T1-weighted sequences reaching the bone cortex compatible with fracture. No alterations in the femoral head were compatible with avascular necrosis”. The patient was discharged with indications to perform a CT scan and a new orthopedic outpatient visit. The CT scan was carried out a few days later and showed an area of bone rarefaction with a vertical course referable to the finding described in MRI and an incomplete fracture in subcapital region. The patient was treated conservatively with oral therapy. The patient took ibandronic acid 150 mg, 1 tablet per month for two months. After the first month the painful symptoms had already disappeared. At a subsequent 3-month follow-up, the patient was completely healed with a complete return to normal daily activities.


Case report 2
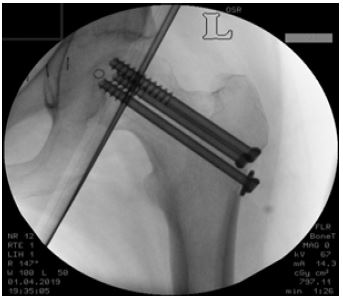
The second case report we present relates the history of a 36-year-old pregnant patient with a mute family history and with a previous history of appendectomy and vocal cord polypectomy. At 36 weeks + 5 days of gestational age, the patient went to the orthopedics outpatient clinic for left coxalgia which has started one month before and gradually had increased. After carefully checking her medical history and examining her hip, trochanteric bursitis was diagnosed. During the outpatient orthopedic visit, the bursitis was treated with corticosteroid + lidocaine local injection and the orthopedist asked for a MRI in case of persistence of hip pain. After a few days the patient went to the emergency room due to the onset of pain in the side and left lower limb. Vital parameters were normal, she was apyretic. Her general physical examination was normal. She was discharged after gynecological evaluation due to the absence of complications. The hypothesis was that the patient had low back pain caused by pregnancy. A week later she went again to the E.R. for accidental fall with possible abdominal impact. An x-ray was obtained and it showed a fracture of the left femoral neck. After a collegial decision between the orthopedic surgeon and the gynecologist she agreed to give birth and afterwards to treat the fracture. The osteosynthesis was obtained with three cannulated screws. After 4 days of hospitalization the patient was discharged with prohibition to bear any weight on the left limb for 40-50 days. The fracture of the femoral neck might have been determined by TOH.

References
- Van Wagenen, Pritchard, Taylor. Transient osteoporosis of the hip: A case report. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3661178/
- K Asadipooya, L Graves, LW Greene. Transient osteoporosis of the hip: Review of the literature.
- Frederico Paiva, Nuno Simões, David Pereira, and Nuno Borralho. Idiopathic Transient Osteoporosis during Pregnancy – Report of a Clinical Case.
- Marco Paoletta, Antimo Moretti, Sara Liguori, Matteo Bertone, Giuseppe Toro and Giovanni Iolascon. Transient osteoporosis of the hip and subclinical hypothyroidism: An unusual dangerous duet? Case report and pathogenetichypothesis.
- Philippe Hernigo, Sibylle Jamma, Jacques Paria, Charles Henri Flouzat-Lachaniett, Arnaud Dubor. Hip osteonecrosis and pregnancy in healthy women. https://pubmed.ncbi.nlm.nih.gov/29279951/
- Crespo E, Sala D, Crespo R, Silvestre A. Transientosteoporosis. https://europepmc.org/article/med/11725563
- Mesut Mutluoglu, Guner Sonmez, Ali Kemal Sivrioglu, Hakan Ay. There may be a role for hyperbaric oxygen therapy in transient osteoporosis of the hip. https://pubmed.ncbi.nlm.nih.gov/23162969/
- Curtiss Paul H; Kincaid William E. Transitory Demineralization of the Hip in Pregnancy. A Report of Three Cases.
- TD Brown, DR Pedersen, KJ Baker, RA Brand. Mechanical consequences of core drilling and bone-grafting on osteonecrosis of the femoral head.