
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Computed tomography pattern of severe cerebral
amyloid angiopathy in the acute phase of stroke
care: what should we do?
Gaia Sirimarco1*; Benoit Wicki1; Stefania Nannoni1; Jean Philippe Brouland2; Jonathan Rosand3; Patrik Michel1
1Stroke Center, Neurology Service, Department of Clinical Neurosciences, Centre Hospitalier Universitaire Vaudois (CHUV) and University of Lausanne, Lausanne, Switzerland.
2Department of Pathology, Centre Hospitalier Universitaire Vaudois (CHUV) and University of Lausanne, Lausanne, Switzerland.
3JP Kistler Division of Neurocritical Care and Emergency Neurology, Center for Genomic Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, USA.
*Corresponding Author : Gaia Sirimarco
Stroke Center, Neurology Service, Department of Clinical Neurosciences, Centre. Hospitalier Universitaire Vaudois (CHUV). Rue du bugnon 46, 1011 Lausanne, Switzerland.
Email: Gaia.Sirimarco@chuv.ch
Received : Nov 16, 2022
Accepted : Dec 19, 2022
Published : Dec 26, 2022
Archived : www.jcimcr.org
Copyright : © Sirimarco G (2022).
Abstract
Background: Intracerebral hemorrhage is a complication of thrombolytic therapy in stroke patients. Furthermore, Cerebral Amyloid Angiopathy (CAA), which itself can cause hemorrhage, may be a risk factor for thrombolysis-related intracerebral hemorrhage. However, only few data are available on this setting. We describe a case of a thrombolysis-related intracerebral hemorrhage in a patient with a diagnosis of CAA and its radiological features, to help physicians in the decision-making process.
Case presentation: A 76-year-old woman presented to the emergency department with acute global aphasia, leading to the suspicion of an acute stroke. A Non-Contrast Computed Tomography Scan (NNCT) excluded a hemorrhagic stroke and the patient was treated by intravenous thrombolysis. Towards the end of thrombolysis infusion, the patient rapidly worsened with a decrease in vigilance. The infusion was stopped after 55 min and a control CT scan was immediately performed, exposing multifocal hemorrhagic transformation, predominantly in the posterior areas. We reviewed the admission CT scan that showed bilateral posterior hypodensities.
The autopsy revealed a Cerebral Amyloid Angiopathy (CAA) type 1. CAA may play a crucial role in the development of thrombolysis-related hemorrhage, especially in patients with multiple lobar micro bleeds.
Conclusions: Our case suggests that in the presence of such a NCCT features, a suspicion of CAA should be included in the differential diagnosis and physicians should consider refraining from thrombolytic therapy. Thereafter, an MRI may help to clarify etiology to better guide patient care in this setting.
Keywords: Cerebral amyloid angiopathy; Thrombolysis-related haemorrhage; Intracerebral hemorrhage; Acute stroke; Intravenous thrombolysis; Cerebral computed tomography.
Abbreviations: CAA: Cerebral Amyloid Angiopathy; NNCT: Non-Contrast Computed Tomography Scan.
Citation: Sirimarco G, Wicki B, Nannoni S, Broulandd JP, Rosand J, et al. Computed tomography pattern of severe cerebral amyloid angiopathy in the acute phase of stroke care: What should we do? J Clin Images Med Case Rep. 2022; 3(12): 2214.
Background
Intracerebral hemorrhage is a well-known complication of intravenous thrombolysis for acute ischemic stroke. On the other hand, Cerebral Amyloid Angiopathy (CAA) is an important cause of cerebral hemorrhage, especially in elderly patients [1]. Furthermore, there is increasing evidence that CAA may be a risk factor for thrombolysis-related intracerebral hemorrhage in the acute ischemic stroke management [2]. Nevertheless, few data are available in the emergency setting. We describe a case of a thrombolysis-related intracerebral hemorrhage in a patient with a histological diagnosis of CAA and its radiological features on CT scan to guide physicians in the decision-making process.
Case presentation
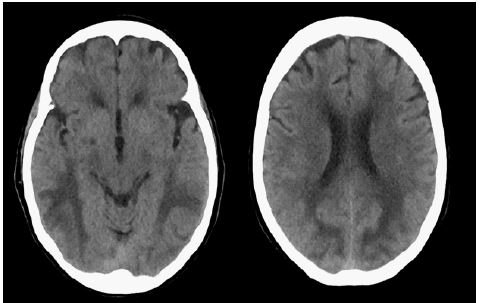
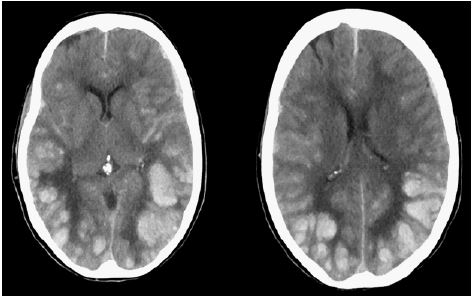
A 76-year-old woman presented with acute global aphasia in an emergency setting, leading to the suspicion of an acute stroke. She had no cardiovascular risk factors but showed slight cognitive decline over the last 18 months in the medical history and a positive familial history of Alzheimer disease. The Non-Contrast Computed Tomography Scan (NNCT) excluded a hemorrhagic stroke and the patient was treated by intravenous thrombolysis 4 h 23 minutes after symptoms onset (Figure 1). Towards the end of thrombolysis infusion, the patient rapidly worsened with a decrease in vigilance. The thrombolysis infusion was stopped after 55 minutes and a control CT scan was immediately performed, showing multifocal hemorrhagic transformation predominantly in the posterior areas (Figure 2). We reviewed the admission CT scan that identified bilateral posterior hypodensities, mainly of the white matter.
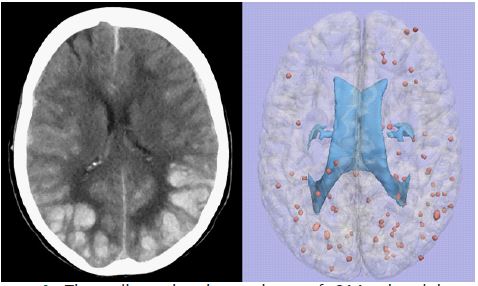
Based on the medical history of a cognitive impairment and the diffuse and severe edema on the initial CT (Figure 1) we suspected an inflammatory-related form of CAA [3-5]. A postmortem examination of the brain and leptomeninges showed deposition of amyloid in leptomeningeal and cortical vessel walls confirming a CAA type 1 but did not show inflammation (Figure 3A-B). The distribution of hemorrhages in our patient well matches a previous description of the pattern of spontaneous hemorrhages in 59 CAA patients [6] (Figure 4).
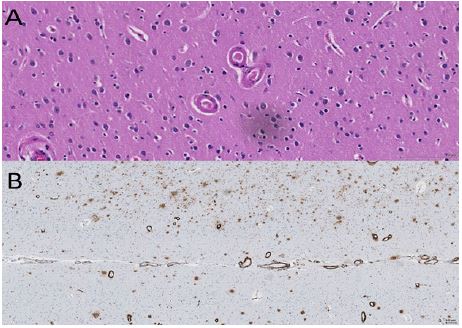
B: Immunostaining showing vascular amyloid-β deposits.
Discussion and conclusion
There is some evidence that CAA may play a role in the development of thrombolysis-related hemorrhage, especially in patients with multiple lobar microbleeds [2,7]. However, it is difficult to make a definitive diagnosis of CAA without pathological examination of the brain tissue. Recent advances in brain imaging techniques may help to provide the diagnosis of ‘probable CAA’, especially certain MRI sequences [8]. However, CT scan is often the initial investigation as it is widely available in emergency departments. Little is known about the radiological features of CAA on CT scan, except for lobar hemorrhage. In this respect, in case of atypical NCCT features such as a diffuse and severe cerebral edema, predominantly in the posterior regions and a history of cognitive decline, the CAA should be considered in the differential diagnosis. In this case, it is advisable to abstain from using thrombolytic therapy. Subsequently, a prompt MRI can be helpful to clarify etiology and better guide patient management.
Declarations
Ethics approval not applicable.
Data are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests.
No funding to declare.
Authors’ contributions: GS: study concept, data collection and interpretation, literature review, preparation of manuscript; SN: data collection and interpretation, literature review and critical revision of the manuscript; BW: data collection and critical revision of the manuscript; JPB: anatomopathologic analysis of cerebral tissues and critical revision of the manuscript; JR: revision of the scientific contents of the manuscript; PM: study concept and critical revision of the manuscript. All authors read and approved the final manuscript.
Acknowledgements: We thank Melanie Price Hirt for English language correction and editing.
References
- Bhomraj Thanvi, Tom Robinson. Sporadic cerebral amyloid angiopathy—An important cause of cerebral haemorrhage in older people. Age and Ageing. 2006; 35: 565–571.
- Mark O McCarron and James AR Nicoll. Cerebral amyloid angiopathy and thrombolysis related intracerebral haemorrhage. Lancet Neurol. 2004; 3: 484–492.
- Kong Khi Chung, Neil E Anderson, David Hutchinson, Beth Synek, P Alan Barber, et al. Cerebral amyloid angiopathy related inflammation: Three case reports and a review. J Neurol Neurosurg Psychiatry. 2011; 82: 20-26.
- Carlo Salvarani, Morris JM, Caterina Giannini, Brown RD Jr, Teresa Christianson, et al. Imaging Findings of Cerebral Amyloid Angiopathy, Ab-Related Angiitis (ABRA), and Cerebral Amyloid Angiopathy–Related Inflammation. A Single-Institution 25-Year Experience. Medicine. 2016: 95: e3613.
- Aimen Moussaddy, Ariel Levy, Daniel Strbian, Sophia Sundararajan, France Berthelet, et al. Inflammatory Cerebral Amyloid Angiopathy, Amyloid-β–Related Angiitis, and Primary Angiitis of the Central Nervous System. Similarities and Differences. Stroke. 2015; 46: e210-e213.
- Jonathan Rosand, Alona Muzikansky, Ashok Kumar, Wisco JJ, Eric E, et al. Spatial Clustering of Hemorrhages in Probable Cerebral Amyloid Angiopathy. Ann Neurol. 2005; 58: 459–462.
- Andreas Charidimou, Puneet Kakar, Zoe Fox, David J Werring. Cerebral microbleeds and the risk of in tracerebral haemorrhage after thrombolysis for acute ischaemic stroke: Systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2013; 84: 277–280.
- Rohit Sharma, Stephanie Dearaugo, Bernard Infeld, Richard O’Sullivan, Richard P Gerraty. Cerebral amyloid angiopathy: Review of clinic radiological features and mimics. Journal of Medical Imaging and Radiation Oncology. 2018; 62: 451–463.