
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
An unusual presentation of a lymphatic malformation in an upper limb
Rebeca Tenajas1*; Pablo Benavente2; Almudena Orois3; David Miraut4
1Family Medicine Department, Arroyomolinos Community Health Centre, Spain.
2Orthopaedic Surgery and Traumatology Department, Hip and Knee Unit, Rey Juan Carlos Hospital, Móstoles, Spain.
3Orthopaedic Surgery and Traumatology Department, Upper Limb Unit, Fuenlabrada Hospital, Fuenlabrada, Spain.
4Advanced Healthcare Technologies, GMV, Tres Cantos, Spain.
*Corresponding Author : Rebeca Tenajas
Family Medicine Department, Arroyomolinos Community Health Centre, Spain.
Email: rebeca.tenajas@salud.madrid.org
Received : Nov 21, 2022
Accepted : Dec 22, 2022
Published : Dec 29, 2022
Archived : www.jcimcr.org
Copyright : © Tenajas R (2022).
Abstract
In this case report, we discuss the presentation, physical examination, imaging studies, and diagnosis of a rare vascular lymphatic malformation in the upper limb of a 3-year old child. Vascular lymphatic malformations are uncommon conditions, which can be misidentified as malignant tumours in children at first glance. The image study is essential to identify them and decide the best treatment strategy in each situation.
Keywords: Lymphatic abnormalities; Lymphatic malformation; Lymphangioma; Ultrasonography; Infant.
Abbreviations: LVM: Lymphatic Vascular Malformation.
Citation: Tenajas R, Benavente P, Orois A, Miraut D, et al. An unusual presentation of a lymphatic malformation in an upper limb. J Clin Images Med Case Rep. 2022; 3(12): 2221.
Introduction/background
Vascular malformations are rare disorders associated to irregularities in blood vessel development. Lymphatic Vascular Malformations (LVM) are usually congenital lesions consisting of small conduits and vesicles of different size caused by lymph fluid accumulation.
LVMs are frequently asymptomatic. They are already present at birth, but they are usually not clinically evident until early childhood, when they may enlarge. LVMs get infiltrated across multiple tissue planes including internal organs, joints, bones, skeletal muscle, and subcutaneous fat. The involvement of deep structures is underestimated on clinical examination. Medical image studies are the key to diagnose LVMs and decide the best treatment procedure.
Report of a case
An otherwise healthy 3-year-old school girl visited the Community Health Centre on the same day that her parents noted the presence of a deformity in the distal region of the left humerus. The patient’s past medical records were unremarkable: the third of four siblings, without previous medical or surgical history, full vaccination schedule. She has a healthy mother, age 41 years.
She denied any constitutional symptoms such as fever, chills, night sweats, weight loss, or fatigue. There were no mobility limitations, neither reported trauma.
Physical examination revealed a large, easily palpable, elongated, slightly tender mass that extended approximately 4 x 3 cm, inside which a rounded lesion with the same soft consistency measuring 2 x 2 cm. There was no palpable associated lymphadenopathy. The deformation was not painful on palpation.
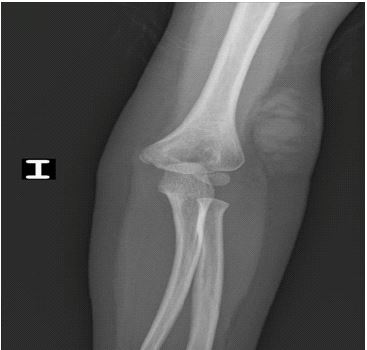
An ultrasound scan of the region was initially requested to the Hospital, but the examination had a delay of three months for non-urgent cases. Instead, it was decided to schedule an X-ray of the upper limb, which could be performed within a week. The radiographic images, in Figures 1 and 2, showed a globular mass located in the distal third of the forearm affecting the soft tissues. Given the findings in the X-ray images, it was recommended to continue the study with an ultrasound scan or magnetic resonance imaging.

Based on the suspicion of the possible presence of a malignant tumour, the patient was sent to the emergency service of the referral hospital where an ultrasound scan was performed. This new diagnostic examination ruled out malignancy, revealing the presence of a rare lymphatic vascular malformation.
The following is a brief review of the ultrasound findings in this case.
Lymphatic vascular malformations are considered to be low-flow vascular malformations as they lack arterial elements. In addition to lymphatic malformations, low-flow lesions also include venous, capillary, mixed and adipose vascular malformations [1,2].
Although the exact cause of lymphatic malformation is not known, it seems that this condition is more common in babies of older mothers. The incidence is estimated to be 1/4000 live births, with no differentiation by race or gender [3].
In spite of its uncommon nature, lymphatic malformations are the second most prominent type of vascular malformation, after venous malformations. They mostly appear in the neck (70-80%), especially in the posterior cervical triangle area, and the axillary region (20%). Lymphatic malformations in the exextremities, like this clinical case, are quite exceptional
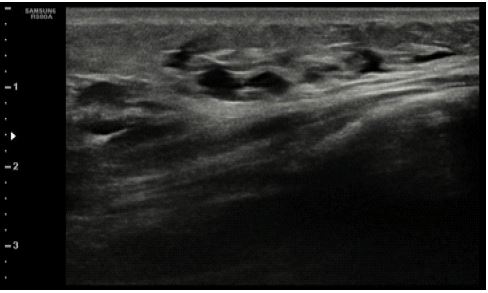
Most lymphatic malformations are identified in the first two years of life. Upon physical exam, they present as normal temperature, nonpulsatile, noncompressible, smooth, soft tissue masses with a rubbery consistency. Lymphatic malformations are composed by chyle-filled cysts lined by flat endothelial cells, they are surrounded by thickened smooth muscle, usually separated by fibrous septa and isolated from the normal draining lymphatic channels, as it can be distinguished in the ultrasound image (Figure 3). According to their size they can be classified as macrocystic or microcystic. They may be associated with infection or haemorrhage, in which case the lesion becomes larger [1].
The protocol for these lesions in children involves close observation for changes in size and possibility of infection [4,5].
The case under study is classified as a microcystic lesion in soft tissue of the upper limb. The ultrasound image (Figure 3) of this set of small cysts is hyperechoic with posterior enhancement, with no flow inside. Due to the size of the lesion, no further imaging studies were performed. Therefore, it has been decided to observe the progression of the lesion as the child grows.
Discussion
Vascular lymphatic malformations are rare, benign masses that caused by abnormal lymphatic system development. Diagnosis of lymphatic malformations usually requires advanced imaging. Determining which imaging modality to choose is not easy, it strongly depends on expected severity and resource availability. Ultrasound helps to visualize cystic structures but lacks the ability to reliably determine mass etiology. Computed tomography and magnetic resonance images reveal better identifying features, but they may require sedation for taking images in children. Therefore, these image modalities are preferred for surgical planning of these lesions.
The decisions regarding treatment strategies will depend on associated symptom and location. Complete resection may not be possible due to microvasculature of the mass near essential organs or the resulting reduction of patients’ physical functions. As far as this condition affects children, alternative methods must be considered [6].
Conclusion
Vascular lymphatic malformations are uncommon entities. Recognizing a vascular malformation from other kind of tumours is a crucial step in terms of patient management. Certain lymphatic lesions can also be the hallmark of certain rare vascular syndromes. In the presence of any lesion compatible with a vascular lesion, it is necessary to complement the exploration with an imaging study, initially an ultrasound exam. It is important for general practitioners, emergency physicians, and radiologists to be familiar with these lesions and their imaging findings.
Declarations
Acknowledgments: We thank the parents’ patient for granting permission to publish the clinical images.
Conflict of interest disclosures: None reported.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
References
- Abernethy LJ. Classification and imaging of vascular malformations in children. European radiology. 2003; 13: 2483-2497.
- Puig S, Casati B, Staudenherz A, Paya K. Vascular low-flow malformations in children: current concepts for classification, diagnosis and therapy. European Journal of Radiology. 2005; 53: 35-45.
- Gallagher JR, Martini J, Carroll S, Small A, Teng J, et al. Annual prevalence estimation of lymphatic malformation with a cutaneous component: Observational study of a national representative sample of physicians. Orphanet Journal of Rare Diseases. 2022; 17: 1-7.
- Bagrodia N, Defnet AM, Kandel JJ. Management of lymphatic malformations in children. Current opinion in Pediatrics. 2015; 27: 356-363.
- Kulungowski AM, Patel M. Lymphatic malformations. Seminars in Pediatric Surgery. 2020; 29.
- Mäkinen T, Boon LM, Vikkula M, Alitalo K. Lymphatic malformations: genetics, mechanisms and therapeutic strategies. Circulation Research. 2021; 129: 136-154.