
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
An incidentally detected Partial Anomalous Pulmonary
Venous Connection (PAPVC) into supra hepatic
IVC- Scimitar syndrome: A case report
Mahesh Gudelli*; Mallu Gangadhar Reddy; M Sravya
Consultant Interventional Pulmonologist, Yashoda Hospital, Secunderabad, Telangana 500017, India.
*Corresponding Author : Mahesh Gudelli
Pulmonary Medicine, Consultant Interventional Pulmonologist, Yashoda Hospital, Secunderabad, Telangana 500017, India;
Ph: +918897976190;
Email: maheshg28@gmail.com
Received : Nov 29, 2022
Accepted : Dec 23, 2022
Published : Dec 30, 2022
Archived : www.jcimcr.org
Copyright : © Gudelli M (2022).
Abstract
Anomalous Pulmonary venous connection is drainage of one or more pulmonary veins outside of left atrium. Anomalous Pulmonary Venous Connection is most common on Left side left upper pulmonary vein drains directly into left innominate vein to ultimately drain into right atrium. Right side Partial Anomalous venous drainage can be into Superior Vena Cava, Right Atrium, Innominate vein or rarely Inferior Vena Cava. Of particular interest is PAPVC to IVC where it can appear as SCIMITAR SIGN with Dextra-position of Heart. It is generally associated with Congenital Heart Defects. Here, Anomalous Venous Drainage is partial from Right Upper lobe tracing along fissure and draining into Supra Hepatic IVC with accessory fissure and Dextraposition of Heart. Patient does not have any Congenital Heart defects.
Citation: Gudelli M, Reddy MG, Sravya M. An incidentally detected Partial Anomalous Pulmonary Venous Connection (PAPVC) into supra hepatic IVC- Scimitar syndrome: A case report. J Clin Images Med Case Rep. 2022; 3(12): 2222.
Case report
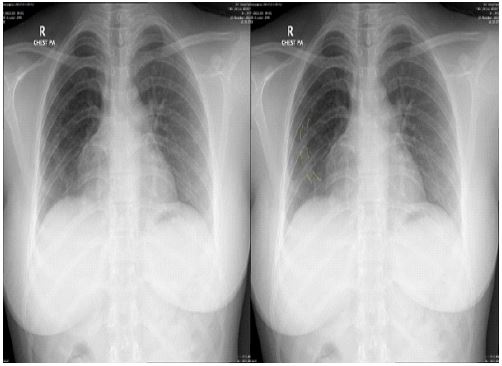
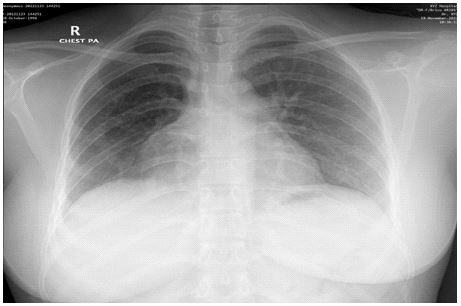
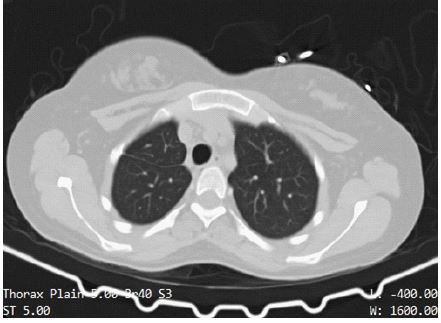
A 28 year old female came with accidental inhalation of steam/unknown gas with symptoms of cough, breathlessness and wheezing. Her oxygen saturation at presentation was 98% with all other vitals in normal range. She was evaluated with Chest X-Ray which showed abnormal Curvilinear opacity on Right side with Dextraposition of heart (Figures 1,2). CECT Chest was further done for evaluation which showed accessory fissure on right side with anamolous Pulmonary vein of Right upper lobe draining along the fissure into Supra Hepatic Inferior Vena Cava (IVC) (Figures 3,4,5). 2D Echocardiography was done which showed no Congenital Heart defects. Her Oxygen Saturaion was within normal range all the time. It is a rare case of Partial Anamolus Pulmonary Venous Connection of Right Upper Lobe into IVC which presents as Scimitar Syndrome but Anamolus Pulmonary vein was Draining along the fissure. Liver function tests are normal and there is no Hepatomegaly.


Discussion
In a Normal Heart, Oxygenated Blood is carried from Lungs into Left atrium via four or more pulmonary veins and deoxygenated blood from systemic circulation drains into right atrium via superior vena cava and Inferior vena cava. In Partial Anamolus Venous Connection, one or more pulmonary veins but not all drain into Right atrium directly or Via systemic veins [1]. Incidence of PAPVC is reported at 0.7% [2].
Anomalous Pulmonary Venous Connection is most common on Left side left upper pulmonary vein drains directly into left innominate vein to ultimately drain into right atrium [1]. PAPVC can be directly into Right atrium or via other systemic veins like Innominate vein, SVC or IVC.
Scimitar Syndrome is a variant of PAPVC comprises a part of or the entire or part of the right lung being drained by right pulmonary veins that connect to the IVC. The affected lung segments are often hypoplastic or has bronchial anomalies [3]. This syndrome can be associated with other cardiac anomalies such as atrial septal defects and aortopulmonary collaterals. Affected infants have a poorer clinical course as compared to affected adults and children. Most infants may have pulmonary hypertension. In chest radiographs, the anomalous draining vein can be seen parallel to the right heart border, giving the appearance of a Turkish sword (“scimitar”) [4]. Most of the adult patients are asymptomatic.
Here, an young female presented with inhalational injury for which Chest X-Ray was done which showed abnormal curvilinear opacity or blood vessel on Right side with Dextraposition of heart and CECT Chest showed Right lung accessory fissure with slight loss of lung volume and abnormal/anamolous Pulmonary vein from Right upperlobe draining along the fisure into Supra Hepativ IVC. 2D-Echo showed no Congenital heart defects. Blood vessel on contrast imaging showed “Scimitar sign”. Patient was asymptomatic and peculiar features includepresence of accessory fissure, Dextroposition of heart, loss of right lung volume which was insignificant without any other bronchial abnormalities.
Diagnosis of Scimitar syndrome can be done by Presence of Scimitar shadow on Chest X-Ray, Magnetic Resonance Imaging, Contrast CT Chest or Multidetector CT scan[5].
Scimitar Syndrome is mostly asymptomatic in adults which presents with Right sided hypoplastic lung with associated bronchovascular abnormalities and abnormally draining one or more pulmonary veins from whole or part of right lung into IVC [1,6].
Conclusion
Scimitar Syndrome is a Partial Anomalous Pulmonary Venous Connection on Right side which is very rare. It can be suspected on Chest X-Ray with presence of “Scimitar sign” on right side with hypoplastic Right lung with Ipsilateral Shift of Cardiac opacity. 2D Echocardiography must be performed in all individuals with Scimitar Syndrome to assess for any Congenital Heart Defects. In Adults, Scimitar syndrome may be of Benign nature with no symptoms. Magnetic Resonance Imaging, Multidetector CT scan or CECT Chest are useful investigation modalities for confirmation of Scimitar syndrome or PAPVC. In asymptomatic individuals, no treatment is necessary but should be followed up closely as Right-to-Left shunt is not significant to cause Hypoxemia or Cyanosis.
References
- Konduri A, Aggarwal S. Partial and Total Anomalous Pulmonary Venous Connection. Stat Pearls 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560707/
- Lapa T, Vedelago J, Kim H, Patrick E. Case Report: An unusual constellation of congenital malformations in a single patient including partial anomalous pulmonary venous return, persistent left superior vena cava, aberrant pulmonary fissure, anomalous aortic arch, tracheal diverticulum and annular pancreas. BMJ Case Rep. 2014; 2014. Available from: /pmc/articles/PMC4216892/
- Gao YA, Burrows PE, Benson LN, Rabinovitch M, Freedom RM. Scimitar syndrome in infancy. J Am Coll Cardiol. 1993; 22: 873–882. Available from: https://pubmed.ncbi.nlm.nih.gov/8354827/
- Huddleston CB, Exil V, Canter CE, Mendeloff EN. Scimitar syndrome presenting in infancy. Annals of Thoracic Surgery. 1999; 67: 154–159.
- Nikolaeva E v. Multidetector Computer Tomography (MDCT) in diagnostics of Partial Anomalous Pulmonary Vein Connection (PAPVC) and Scimitar syndrome. 2015; Available from: https://epos.myesr.org/poster/esr/escr2015/P-0036
- Hegde M, Manjunath SC, Usha MK. Isolated Partial Anomalous Pulmonary Venous Connection: Development of Volume Overload and Elevated Estimated Pulmonary Pressure in Adults Journal of Clinical Imaging Science. Journal of Clinical Imaging Science. 2022; 2019. Available from: www.clinicalimagingscience.org