
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Moebius syndrome in association with hypogonadotrophic hypogonadism and focal motor demyelinating peripheral neuropathy with persistent conduction blocks
Francesco Piccione1; Lisa Ragazzo2; Daniele Coraci2; Stefano Masiero2; Paolo Tonin3; Antonio Cerasa3,4,5*
1Neurorehabilitation Unit Azienda Ospedale Università Padova, Italy.
2Department of Neuroscience, Physical Medicine and Rehabilitation, University of Padova, Italy.
3S’Anna Institute, 88900 Crotone, Italy.
4Institute for Biomedical Research and Innovation (IRIB), National Research Council of Italy (CNR).
5Pharmacotechnology Documentation and Transfer Unit, Preclinical and Translational Pharmacology, Department of Pharmacy, Health Science and Nutrition, University of Calabria, 87036 Arcavacata, Italy.
*Corresponding Author : Antonio Cerasas
IRIB-CNR, Messina, Italy.
Email: Antonio.cerasa76@gmail.com.
Received : Dec 06, 2022
Accepted : Dec 26, 2022
Published : Jan 02, 2023
Archived : www.jcimcr.org
Copyright : © Cerasa A (2023).
Keywords: Moebius syndrome; Hypogonadotrophic hypogonadism; EMG.
Citation: Piccione F, Ragazzo L, Coraci D, Masiero S, Cerasa A, et al. Moebius syndrome in association with hypogonadotrophic hypogonadism and focal motor demyelinating peripheral neuropathy with persistent conduction blocks. J Clin Images Med Case Rep. 2023; 4(1): 2223.
Introduction
Congenital, non-progressive facial paralysis and a restricted abduction of one or both eyes are symptoms of Moebius Syndrome (MBS) [1]. Peripheral neuropathy, Kallmann syndrome, intellectual disability, and social impairment are also evident in a subgroup of people with inherited congenital facial nerve atrophy and oculomotor nerve palsy [2]. Moebius syndrome with hypogonadotropic hypogonadism is associated with progressive peripheral neuropathy and is often axonal and occasionally demyelinating [3-6]. Electromyography in this uncommon clinical type shows high amplitude motor unit potentials with reduced recruitment in the leg muscles when an axonopathy is present. Electroneurography has shown that motor and sensory nerves exhibit lower amplitudes, different axonal properties, and slightly slower conduction velocities [2-7]. We describe, for the first time, a case of a patient with MBS along with chronic multifocal demyelinating motor neuropathy and persistent conduction blocks due to hypogonadotropic hypogonadism.
Case history
A seventeen-year-old male subject who had previously been diagnosed with MBS for congenital paresis of both VII cranial nerves and limited eye abduction displayed growing ankle dorsiflexion weakness during childhood, which was more pronounced on the left side. There were no hints that the neuropathy was inherited. Additionally, the patient had anosmia and hypogonadotropic hypogonadism (Kallmann syndrome). An equinovarus deformity of the foot and ankle as well as bilateral drop feet with steppage gait were discovered during a physical examination before admission to the neurorehabilitation ambulatory unit. In the anterior-lateral compartments of the legs, there were signs of muscle hypotony and partial atrophy, which were more obvious on the left side. Before the neurorehabilitation examination, untrained doctors working in a general medical facility treated stiffness in the left calf muscles with an ineffective injection of botulinum toxin A (left Gastrocnemius caput medialis and Tibialis Posterior muscles). After this therapy, the patient reported worsening muscular trophism throughout the entire left leg and no improvement in their motor impairments. The subject displayed no abnormalities in breathing or swallowing and showed no evidence of upper motor neuron involvement.
Electrodiagnostic studies
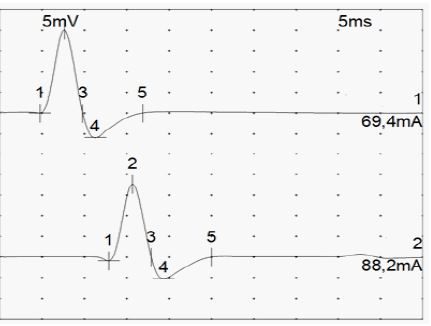
The following common approaches are part of the neurophysiological protocol used in the electrodiagnostic examinations carried out in the Neurorehabilitation Unit EMG Lab of General Hospital - University of Padua. Blink reflex, motor conduction studies of the seventh cranial nerve, medial, ulnar, peroneal, and tibialis posterior motor nerves with the registration of F waves, medial, ulnar, and sural sensory nerve conduction studies, and needle electromyography of the face (Orbicularis oculi and oris muscles), limbs, and heart are all examples of such studies (Deltoid, Abductor pollicis brevis, first dorsal Interosseus, Tibialis anterior, Peroneus longus, Gastrocnemius caput medialis, Tibialis Posterior, Extensor digitorum brevis). Exams verified earlier findings that there was no motor unit activation in the face muscles’ EMG or absence of blink and VII cranial nerve motor nerve responses. Chronic neurogenic EMG findings of the bilateral Tibialis anterior and Peroneus longus were found by limb needle electromyography. Additionally, the left Gastrocnemius caput medialis and the left Tibialis Posterior displayed mild neurogenics (previously injected with botulinum toxin A). Electroneurography showed a small drop in motor conduction velocity in the right Tibialis posterior nerve and a bilateral partial conduction block in the Peroneal nerves at the fibular head (cMAP amplitude and area decline) (See Table 1 and Figures 1, 2).
Table 1: The course of endoscopic treatments.
| Nerve | Muscle | Latency | Amplitude | Rel Amp | Segment | Distance | Lat Diff | Velocity | Rel Vel | Area 1-5 |
|---|---|---|---|---|---|---|---|---|---|---|
| ms | mV | % | mm | ms | m/s | % | mVms | |||
| Left Peroneal - EDB | ||||||||||
| Ankle | EDB | 5.23 | 0.9 | 100 | Ankle - EDB | 5.8 | ||||
| Fibular Head | EDB | 12.46 | 1.3 | 135 | Fibular Head - Ankle | 300 | 7.23 | 41 | 100 | 6.8 |
| Popliteal fossa | EDB | 17.29 | 0.3 | 20.5 | Popliteal fossa - Fibular Head | 120 | 4.83 | 25 | 59.8 | |
| Right Peroneal - EDB | ||||||||||
| Ankle | EDB | 4.63 | 3.3 | 100 | Ankle - EDB | 13.5 | ||||
| Fibular Head | EDB | 10.98 | 3.8 | 115 | Fibular Head - Ankle | 330 | 6.35 | 52 | 100 | 18.5 |
| Popliteal fossa | EDB | 12.90 | 3.5 | 92.1 | Popliteal fossa - Fibular Head | 80 | 1.92 | 42 | 80.4 | 15.4 |
| Left Tibialis - AH | ||||||||||
| Ankle | AH | 3.21 | 20.6 | 100 | Ankle - AH | 80 | 67.5 | |||
| Popliteal fossa | AH | 11.92 | 17.9 | 87 | Popliteal fossa - Ankle | 400 | 8.71 | 46 | 100 | 66.5 |
| Right Tibialis - AH | ||||||||||
| Ankle | AH | 4.71 | 20.1 | 100 | Ankle - AH | 80 | 70.5 | |||
| Popliteal fossa | AH | 12.85 | 18.6 | 92.7 | Popliteal fossa - Ankle | 350 | 8.15 | 43 | 100 | 64.6 |

Except for a slightly decreased number of F-Waves induced by stimulation of lower limb motor neurons, all other neurophysiologic parameters in needle EMG, Motor, and Sensory conduction investigations were within normal ranges. After that, during a follow-up appointment, a dorso-lumbar spine MRI ruled out disc herniation or foraminal stenosis at that level crushing the L4 or L5 nerve roots, and a knee ultrasound exam ruled out a common source of peroneal nerve compression at the fibular head.
Discussion
Along with facial and oculomotor congenital paresis [1], the MBS also had bilateral drop feet and a steppage gait. After receiving an untimely injection of botulinum toxin in the left calf muscles during childhood, the patient’s motor skills for walking were delayed and slowly got worse [8]. Electroneurography of the lower limbs revealed focal motor peripheral neuropathy with persisting conduction blockages of the peroneal nerve at the fibular head in this clinical version of Moebius syndrome. In muscles of the anterior-lateral compartments of the legs, needle EMG revealed high amplitude motor unit potentials with reduced recruitment, which is consistent with the existence of dorsiflexor muscle abnormalities. Other myotomes not innervated by the Peroneal nerve exhibit demyelinating aspects of the neuropathy with intact sensitive responses and normal needle EMG findings, according to electrodiagnostic research [2-7]. Only one research has described the co-existence of MBS and focal motor peripheral neuropathy with chronic conduction blocks [3-6]. The findings of this study also aid in the planning of rehabilitation therapy for the syndrome, which includes functional electrical stimulation of the leg muscles in addition to traditional physical therapy and AFO bracing to increase foot dorsiflexion and avoid leg muscle atrophy [8].
References
- Pitner SE, Edwards JE, Mccormick WF. Observations on the pathology of the moebius syndrome. J Neurol Neurosurg Psychiatry. 1965; 28: 362-374.
- Lehky T, Joseph R, Toro C, Wu T, Ryzin CV, et al. Moebius Syndrome Research Consortium. Differentiating Moebius syndrome and other congenital facial weakness disorders with electrodiagnostic studies. Muscle Nerve. 2021; 63: 516-524.
- Baraitser M, Rudge P. Moebius syndrome, an axonal neuropathy and hypogonadism. Clin Dysmorphol. 1996; 5: 351-355.
- Koide Y, Yamashita N, Kurusu T, Kugai N, Kuzuhara S, et al. Association of isolated adrenocorticotropin deficiency with a variety of neuro-somatic abnormalities in congenital facial diplegia (Moebius) syndrome. Endocrinol Jpn. 1983; 30: 499-507.
- Abid F, Hall R, Hudgson P, Weiser R. Moebius syndrome, peripheral neuropathy and hypogonadotrophic hypogonadism. J Neurol Sci. 1978; 35: 309-315.
- Rubinstein AE, Lovelace RE, Behrens MM, Weisberg LA. Moebius syndrome in Kallmann syndrome. Arch Neurol. 1975; 32: 480-502.
- Marciniak C. Fibular (peroneal) neuropathy: Electrodiagnostic features and clinical correlates. Phys Med Rehabil Clin N Am. 2013; 24: 121-137.
- Sackley C, Disler PB, Turner-Stokes L, Wade DT, Brittle N, et al. Rehabilitation interventions for foot drop in neuromuscular disease. Cochrane Database Syst Rev. 2009; 8: CD003908.