
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
The function of pain in the diagnosis of disorders of consciousness: A case report
Maria Daniela Cortese; Lucia Francesca Lucca; Martina Vatrano; Francesco Riganello*
S. Anna Institute, Via Siris 11, 88900 Crotone, Italy.
*Corresponding Author : Francesco Riganello
S. Anna Institute, Via Siris 11, 88900 Crotone, Italy.
Email: francescoriganello@isakr.it
Received : Dec 01, 2022
Accepted : Dec 26, 2022
Published : Jan 02, 2023
Archived : www.jcimcr.org
Copyright : © Riganello F (2023).
Abstract
The correct diagnosis of patients with disorders of consciousness is still challenging. The accurate observation of the behavioral responses in patients with Disorders Of Consciousness (DoC) is crucial to avoid misdiagnosis. We observed changes in the behavioral response in a patient diagnosed with Unresponsive Wakefulness Syndrome/Vegetative State onlyafter nociceptive stimulation, administered following the Nociception Coma Scale indication. This case shows that accurate pain assessment in DoC patients could be crucial to assess covert consciousness content in patients diagnosed as UWS/VS, improving the effectiveness of treatment and rehabilitation path.
Keywords: Disorders of consciousness; Nociception; Pain; Unresponsive wakefulness syndrome; Consciousness.
Citation: Cortese MD, Lucca LF, Vatrano M, Riganello F. The function of pain in the diagnosis of disorders of consciousness: A case report. J Clin Images Med Case Rep. 2023; 4(1): 2224.
Introduction
The correct diagnosis of patients with disorders of consciousness is still challenging [1]. Today the rate of misdiagnosis is still around 30% [2]. The Coma Recovery Scale-Revised (CSR-R) is the gold standard for diagnosing patients with Disorders Of Consciousness (DoC) [3]. While open eyes, basic reflexes, and no behavioral evidence of self or environmental awareness characterize the patient with Unresponsive Wakefulness Syndrome/Vegetative State (UWS/VS), the patient with the diagnosis of a Minimally Conscious State show some minimal or inconsistent signs of awareness, such as visual pursuit, localization to pain, or non-systematic command-following. The accurate observation of the behavioral responses in patients with UWS/VS diagnosis is crucial to avoid misdiagnosis. We observed changes in the behavioral response in a patient with diagnosis of UWS/VS onlyafter nociceptive stimulation, administered following the Nociception Coma Scale indication [4], a scale developed to assess pain in DoC patients.
Case presentation
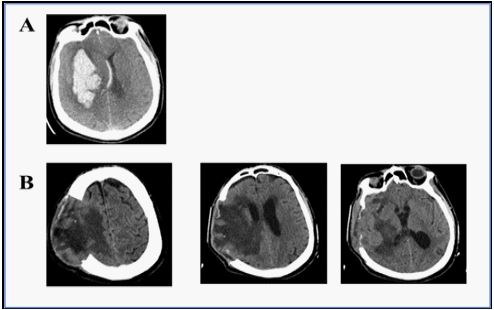
A 74 years-old male patient was hospitalized at S. Anna Institute 22 days after the acute event characterized by right fronto-temporal-parietal craniectomy surgery. The acute event was characterized by an evident and extensive area of blood hyperdensity, of a hemorrhagic nature involving the nucleus-capsular region and at the temporal-parietal-occipital level on the right, the presence of blood flooding of the posterior horns of both lateral ventricles, leftward shift of midline structures, and smoothing of the sulci of the cerebral cortex (Figure 1A). At the admission, the CT of the patient evidenced a slight reduction in the fluid-superfluid density level at the surgical cavity, the reduction of compression on midline structures, with minimal re-expansion of the left ventricular hemisystem. Significantly reduced the amount of pneumocephalus in the bilateral frontal site andthin extra-axial hypodense layer in the right frontal site along the convexity (Figure 1B).
Ten days after the hospitalization in our institute and stabilized his clinical condition, the patient’s level of consciousness was assessed in the psychophysiology lab of the care unit. After a baseline of 10 minutes, the Heart Rate (HR), Galvanic Skin Response (GSR), temperature, and Electrooculogram (EOG) were monitored during the stimulations. The total score of 3 at the CRS-R confirmed the diagnosis of UWS/VS. He did not show any behavioral responses to auditory stimuli (i.e., absence of auditory startle), visual stimuli (i.e., the impossibility of eliciting the eye-opening), and abnormal posturing to the nociceptive stimulus.The behavioral responses to the noxious stimulus were assessed following the NCS procedure. The stimulus was administered to the four limbs by applying a pressure on the nailbed for a maximum of 5 seconds with an algometer and observing the behavioral response for 10 seconds after the noxious stimulus.The patients showed a clear and specific behavioral response only when the stimulus was applied to the left foot with a pressure of 9 Newton,characterized by flection withdrawal, grimace, intelligible verbalization, and a total score of 7.
Compared to the baseline, characterized by an HR of 89 b/m with low variability (8 milliseconds), during the stimulation,the HR variability increased (31 milliseconds) but not its frequency, and the GRS showed significant changes only during the noxious stimulation.
Importantly, in the first phase of the rehabilitation path, the patient showed behavioral responses only immediately after the nociceptive stimulation. Three months after the acute event, he was diagnosed emerged from the MCS condition.
Conclusion
Assessing behavioral responses in patients with the diagnosis of UWS/VS is challenging. This patient represents a paradigmatic case where the absence of evident responsesto the administered stimuli is favorable for a diagnosis of UWS/VS. Nevertheless, the accurate assessment of the behavioral response to the nociceptive stimulation evidencedcovert content of consciousness. Previous studies showed that the behavioral response to the noxious stimuli could precede the change in the level of consciousness in UWS/VS patients [5,6]. However, the individual threshold and clinical variability of pain causes in patients with disorders of consciousness might make the correct assessment of the behavioral response difficult [7,8]. The treatment and management of pain are challenging issues in patients with DOC. The no unanimous consensus about whether non-responsive patients might have a sufferance condition or might feel pain implies increasing ethical questions [9,10].
This case shows that accurate pain assessment in DoC patients could be crucial to assess covert consciousness content in patients diagnosed as UWS/VS, improving the effectiveness of treatment and rehabilitation path.
References
- Giacino JT, Katz DI, Schiff ND. Practice Guideline Update Recommendations Summary: Disorders of Consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Archives of Physical Medicine and Rehabilitation. 2018; 99: 1699–1709.
- Van Erp WS, Lavrijsen JCM, Vos PE. The Vegetative State: Prevalence, Misdiagnosis, and Treatment Limitations. Journal of the American Medical Directors Association. 2015; 16: 85.e9-85.e14.
- Giacino JT, Kalmar K, Whyte J. The JFK Coma Recovery Scale-Revised: Measurement characteristics and diagnostic utility. Archives of Physical Medicine and Rehabilitation. 2004; 85: 2020–2029.
- Riganello F, Cortese MD, Arcuri F. A study of the reliability of the Nociception Coma Scale. Clinical Rehabilitation 2014; 1.
- Cortese MD, Arcuri F, Nemirovsky IE. Nociceptive Response Is a Possible Marker of Evolution in the Level of Consciousness in Unresponsive Wakefulness Syndrome Patients. Frontiers in Neuroscience. 2021; 15. https://www.frontiersin.org/articles/10.3389/fnins.2021.771505 (accessed 26 Jul 2022).
- Cortese D, Riganello F, Arcuri F. The Trace Conditional Learning of the Noxious Stimulus in UWS Patients and Its Prognostic Value in a GSR and HRV Entropy Study. Front Hum Neurosci. 2020; 14.
- Schnakers C, Zasler N. Assessment and Management of Pain in Patients With Disorders of Consciousness. PM & R 2015; 7: S270– S277.
- Sattin D, Schnakers C, Pagani M. Evidence of altered pressure pain thresholds in persons with disorders of consciousness as measured by the Nociception Coma Scale–Italian version. Neuropsychological Rehabilitation. 2018; 28: 1295–310.
- Riganello F, Macrì S, Alleva E. Pain Perception in Unresponsive Wakefulness Syndrome May Challenge the Interruption of Artificial Nutrition and Hydration: Neuroethics in Action. Front Neurol. 2016; 7.
- Fins JJ, Wright MS, Bagenstos SR. Disorders of Consciousness and Disability Law. Mayo Clinic Proceedings 2020; 95: 1732–1739.