
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Delayed leprosy increasing morbidities in disability and neuropathic pain: A case report
*Corresponding Author : Paula M Samosir
Mentikan Public Primary Healthcare, Jln. Prapanca, Mojokerto city, East Java Province 61323, Indonesia.
Phone: +62-8223-584-5480;
Email: paulasamosir94@gmail.com
Received : Dec 05, 2022
Accepted : Dec 28, 2022
Published : Jan 04, 2023
Archived : www.jcimcr.org
Copyright : © Samosir PM (2023).
Abstract
Introduction: Leprosy remains a public health problem in many developing countries, especially, in tropical regions. Even though the prevalence rate of leprosy in Indonesia has decreased, however from 2001 to 2019, there has been an increasing trend of leprosy cases with disabilities. The rate of grade 2 disability cases is an indicator of the effectiveness of leprosy health services, especially in terms of case detection.
Case: We report a case of leprosy which presented with disability and neuropathic pain as consequences of delayed diagnosis. The diagnosis was delayed for 3 years since the first symptoms, disability and severe reversal reaction were present at the time of diagnosis.
Discussion: Delays are associated with higher rates of permanent nerve damage and disability. Misdiagnosis and unawareness of the disease are the main factors that influenced the delayed diagnosis and treatment; thus increasing the risk of morbidities including disability and neuropathic pain.
Conclusion: Early detection and prompt treatment of leprosy are very important to minimize morbidities in leprosy. It is important to raise awareness and knowledge about leprosy in the community and among healthcare providers, particularly in primary healthcare settings.
Keywords: Leprosy; Delayed; Misdiagnosis; Disability; Neuropathic pain.
Citation: Samosir PM. Delayed leprosy increasing morbidities in disability and neuropathic pain: A case report. J Clin Images Med Case Rep. 2023; 4(1): 2227.
Introduction
Leprosy, also known as Hansen’s disease, is a chronic infectious disease that primarily affects peripheral nerves and skin [1]. Leprosy remains a complex public health problem in Indonesia because until now there are still 6 provinces that have not achieved the elimination of leprosy [2]. Elimination of leprosy is challenging because of the treatment delay, difficulty in diagnosis, high transmission, and social stigma [3]. According to the Indonesian Ministry of Health, the prevalence rate of leprosy in Indonesia has decreased, but from 2001 to 2019 there has been an increasing trend of leprosy cases with grade 2 disabilities, with a proportion above 10% [4]. The rate of grade 2 disability cases reflects the effectiveness of leprosy health services. If the rate is high, it is clear that services must be improved, particularly in terms of case detection [1,4].
Delay of diagnosis and treatment are associated with higher rates of permanent nerve damage and disability [5]. It is critical to recognize and treat leprosy and neuritis early in order to avoid further nerve damage and complications, such as disability and neuropathic pain [6]. Disability and neuropathic pain can significantly affect a patient’s quality of life, stigmatization, economic problems and lead to psychological distress [6,7]. Because of the inability to perform differential diagnoses and a lack of specific training, accurate diagnosis of leprosy in primary health care may be more difficult [8]. Patient’s behavior in seeking medical treatment was the other most prominent factor associated with delayed case detection [9]. We will present a case of delayed leprosy in the city of Mojokerto due to misdiagnosis by primary healthcare providers and the patient’s unawareness which resulted in disability and complications of neuropathic pain.
Case
A 37-year-old man from Mojokerto with no known comorbidities presented to the Mentikan Public Primary Health Care with complaints of multiple red patches over his entire body, most noticeable over his face and upper extremities for the last three years. The first lesion began at his forehead as multiple papules then spread to his neck, trunk, and his extremities as multiple patches. The lesions did not accompany by pruritic, numb, or pain sensations, therefore the patient did not go for a check-up because he felt it was not too disturbing. The patient tried self-medications and traditional medicines. He started to complain of reduced sensation on both of his hands and feet two years later. He had made several local primary healthcare visits in Mojokerto since then and given several topical and oral medications but the lesions persisted with no progression.
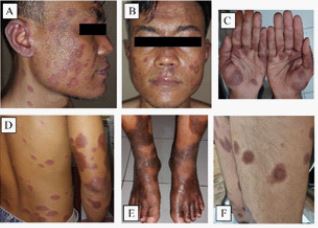
Two months before the visit, the patient noticed that some of the patches were changing and becoming painful. He also complained of weakness on both of his hands and feet. The patches became thickened, there were also new lesions appeared, therefore he decided to get checked by a dermatologist. After being treated for about 2 weeks and there was no improvement, the patient was suggested to take a slit skin smear examination in the public primary healthcare and it showed numerous acid-fast bacilli. The history of a family member suffering from similar symptoms was unclear, but he had a history of working in Madura Island several years ago, where cases of leprosy were found around his workplace. Physical examination revealed multiple erythematous nodules on his forehead and erythematous plaques around the facial area and back of the neck. Both earlobes showed inflammatory infiltration. Multiple skin-colored nodules and erythematous plaques were noticed on the trunk. Multiple erythematous plaques of various sizes with an edematous appearance and well-demarcated raised edges, sparing the central region were found on the upper extremities region. Multiple erythematous and hyperpigmented plaques were also found on the lower extremities region shown in the Figure 1. The blood pressure, heart rate, and temperature are within the normal limit.
He had bilateral enlargement of the ulnar, peroneal communal, and posteriortibial nerves. Nerve pain and tenderness were also present in the examination. There was a decrease of sensation on both of his hands and feet. Examination of voluntary muscle tests on the hands and feet showed weakened muscle strength. Slit-skin smears were performed and showed multiple acid-fast bacilli with a Bacteriological Index (BI) of 2+ and Morphological Index (MI) was 3%. The blood test was normal. With the above-mentioned findings, he was diagnosed as having multibacillary leprosy with severe reversal reaction and grade 1 disability. According to the WHO guideline for leprosy treatment, the patient was treated with MDT regimen, prednisone 40 mg daily subsequently tapered off every 2 weeks, and other symptomatic medication. After 3 months of treatment, the patches started to thin out and became hyperpigmented, pain and tenderness had relieved. However, the numbness and the weakness on his hands and feet remained. Prednisone was continued with a tapering-off dose until discontinued after 4 months of treatment.
On the 11th month of MDT treatment, the patient came with chief complaint of burning, electric, and tingling sensation on his elbow and feet since 2 months ago. The pain was provoked accidentally by exposure to light pressure or friction. The plaques became hyperpigmented and xerotic shown in Figure 2. The pain caused disruption in his daily life and sleep, sometimes he took some medication for pain relief. The patient was assessed as having neuropathic pain by using The Douleurneuropathique 4 Questionnaire (DN4) and obtained a score of 6. The patient was given natrium diclofenac twice a day and continued MDT therapy.

Discussion
Leprosy remains a public health problem in many developing countries and is the leading infectious cause of disability [1]. Leprosy that is not treated immediately causes this disease to develop in a progressive direction causing damage to the skin, nerves, limbs, and eyes [1,9]. In Asia, Africa, Europe, and North America, delays in diagnosis have been reported and are associated with higher rates of permanent nerve damage and disability [5]. Based on a study conducted in Colombia by Cardona and Castro, 30% of newly reported cases have disabilities (grades 1 and 2) at the time of diagnosis. This amount is indicated as a consequence of the delay in the discovery of new cases [10]. Delays can occur in the period between the first symptoms noticed and the first visit to the health care provider, as well as the period between the patient’s first visit to the health care provider until the patient is diagnosed with leprosy [11].
In this case, the patient did not immediately go for a check-up because the patient was not bothered by the skin symptoms, and was related to the patient’s lack of knowledge about leprosy. From the studies in India, it is discovered that most patients were still lacking knowledge about the signs or symptoms of leprosy and therefore ignored them; or thought they would disappear spontaneously [11]. There is also a strong belief in traditional medicine as the first action [12]. Personal factors related to delayed case detection were older age, being male, having a lower perception of disease symptoms, and a lack of knowledge. Stigma was the most frequently mentioned social and community factor correlated to delayed case detection [9].
Two years after the first symptoms were noticed, the patient started to complain of reduced sensation and weakness on both of his hands and feet. He had made several primary care outpatient visits in Mojokerto and was diagnosed with allergic skin, fungal infection, and autoimmune conditions by the primary health care professionals. This incorrect diagnosis allowed the leprosy infection to spread throughout the body and progress the nerve damage. The diagnosis of leprosy in current practice is based on the presence of at least one of the three cardinal signs: (i) loss of sure sensation in pale (hypopigmented) or reddish skin; (ii) thickening of peripheral nerve or (iii) the presence of acid-fast bacilli/AFB in the skin scraping [1].
Primary care in Indonesia is conducted by Public Primary Healthcare/Puskesmas and Primary Care Clinics covering around 86% of total healthcare facilities in Indonesia. Primary care physician plays an important role as a gatekeeper and are responsible for primary screening and conducting comprehensive management including referral management [13]. Recent studies discovered that misdiagnosis was the main healthcare factor related to delay [14]. A study in Brazil about the impact after diagnosis and treatment of leprosy was integrated into the primary healthcare services found that 40% of the patients with leprosy had a higher disability grade at diagnosis, indicating a late diagnosis. These results are probably the consequence of difficulties encountered in diagnosing leprosy in primary healthcareservices without specialized health professionals or adequate laboratory tests [8]. Accurate diagnosis of leprosy in primary care may be more challenging due to inability to do differential diagnoses and a lack of specific training [8,14]. In many nations, its elimination as a public health issue appears to be associated with a lack of practical knowledge among health care providers and as a result, a risk of delayed diagnosis [9].
The patient started treatment 3 years after initial symptoms and was diagnosed with MB leprosy with reversal reaction and grade 1 disability. A study from Bangladesh and Ethiopia showed that patients with delayed diagnosis of more than 1 year have a 10%–15% increase in impairment, and delays of 2 years can result in a 15%–25% increase in impairment. The longer the time from the first symptoms noticed until the start of treatment, the greater the risk of developing a disability due to progressive nerve damage [12]. A severe reversal reaction was discovered when the patient was first diagnosed, however, the reversal reactions may have lasted for several months prior to the patient’s first diagnosis so the treatment for the reaction was delayed. Type 1 reactions result from the activation of cell immunity, expressed clinically by exacerbation of skin and nerve trunk inflammation, leading to sensory and motor alterations. Neuritis is present if an individual has any of the following: Spontaneous nerve pain, paresthesia, tenderness, new sensory or motor impairment [4]. The reaction conditions are the main cause of damage to the nerves and disabilities triggered by leprosy, especially when are not properly diagnosed and treated [1,4]. The diagnosis of reactions requires certain clinical skills; effective treatment requires careful judgment, as the clinical course is rarely straightforward [1,6].
After 11 months of MDT treatment, the patient was having neuropathic pain described by burning, electric, and tingling sensation on his hand and feet. In the absence of biomarkers or other gold standard examination, the diagnosis is initially clinical using Validated clinical instruments for pain screening, such as Neuropathic Symptoms and Signs (LANSS) and Douleurneuropathiqueen 4 questions (DN4) [6,15]. According to a study in Brazil, it was concluded that there was a correlation between neuropathic pain and the degree of disability [15]. However, neuropathic pain itself can cause significant decrease in functional capacity and quality of life regardless of the degree of disability [6]. The majority of patients with neuropathic pain were multibacillary, had physical limitations, and had leprosy reactions [15]. Toh et al (2018) discovered that leprosy-related neuropathic pain was significantly influenced by nerve tenderness and reactions [6]. It is critical to early recognize and treat leprosy and neuritis in order to prevent further nerve damage and neuropathic pain [6,7]. The presence of neuropathic pain can significantly affect a patient’s quality of life and lead to psychological distress.
Conclusion
Early detection and prompt treatment of leprosy are very important. If the symptoms or manifestations of leprosy are not treated immediately, it will increase the risk of morbidity which later have an impact on the patient’s quality of life, stigmatization, and economic problems for patients and their families. Raising community awareness about leprosy would promote early consultation and potentially enhance early case detection. Even though Indonesia’s prevalence rate of leprosy has started to decrease, it is still important to improve the capacity of healthcare providers, especially in primary healthcare settings where they have an important role as a gatekeeper in early case detection.
References
- World Health Organization. Guidelines for the Diagnosis, Treatment and Prevention of Leprosy. Geneva: WHO; 2018.
- Kementrian Kesehatan Republik Indonesia. Mari Bersama Hapuskan Stigma dan Diskriminasi Kusta di Masyarakat [Internet]. Jakarta: Direktorat Jenderal Pencegahandan Pengendalian Penyakit [updated 2022 Jan 31, cited 2022 Oct 16]. Available from: http://p2p.kemkes.go.id/mari-bersama-hapuskan-stigma-dan-diskriminasi-kusta-di-masyarakat/
- Ramona F, Sutrisna EM. Leprosy: An overview of epidemiology and risk factor in Indonesia. J Bio Innov. 2017; 6: 991-995.
- Kementrian Kesehatan RI. Peraturan Menteri Kesehatan Republik Indonesia Nomor 11tahun 2019 tentang Penanggulangan Kusta. Jakarata; 2019.
- Zhang F, Chen S, Sun Y, Chu T. Healthcare seeking behaviour and delay in diagnosis of leprosy in a low endemic area of China. Lepr Rev. 2009; 80: 416–423.
- Toh HS, Maharjan J, Thapa R, Neupane KD, Shah M, et al. Lockwood DNJ. Diagnosis and impact of neuropathic pain in leprosy patients in Nepal after completion of multidrug therapy. PLoS Negl Trop Dis. 2018; 12: e0006610.
- Somar P, Waltz MM, van Brakel WH. The impact of leprosy on the mental wellbeing of leprosy-affected persons and their family members - a systematic review. Glob Ment Health (Camb). 2020; 7:e15.
- Barbieri R, Sales AM, Hacker MA. Impact of a Reference Center on Leprosy Control under a Decentralized Public Health Care Policy in Brazil. PLoS Neglected Tropical Diseases. 2016; 10: e0005059.
- Dharmawan Y, Fuady A, Korfage I, Richardus JH. Individual and community factors determining delayed leprosy case detection: A systematic review. PLOS Neglected Tropical Diseases. 2021; 15: e0009651.
- Cardona N and Castro. Leprosy in Colombia: Post Elimination Stage? Lepr Rev. 2013; 84: 238–274.
- Srinivas G, Muthuvel T, Lal V, Vaikundanathan K, Schwienhorst-Stich E-M, et al. Risk of disability among adult leprosy cases and determinants of delay in diagnosis in five states of India: A case-controlstudy. PLOS Neglected Tropical Diseases. 2019; 13: e0007495–e.
- Van Veen NH, Meima A, Richardus JH. The relationship between detection delay and impairment in leprosy control: A comparison of patient cohorts from Bangladesh and Ethiopia. Lepr Rev. 2006; 77: 356–365.
- Werdhani RA. Medical problem in Asia pacific and ways to solve it: The roles of primary care/family physician (Indonesia Xperience). J Family Med Prim Care. 2019; 8: 1523-1527.
- Dharmawan Y, Fuady A, Korfage IJ, Richardus JH. Delayed detection of leprosy cases: A systematic review of healthcare-related factors. PLOS neglected tropical diseases. 2022; 16: e0010756.
- Del’Arco R, De Oliveira AB, Nardi SM, Paschoal VD. The association between neuropathic pain and disability grades in leprosy. Lepr Rev. 2016; 87: 53-59.