
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Wilkie syndrome, changing perspectives in image visualization
Ronchi Brunela¹*; Peña Gustavo¹; Eede Gabriela²
1Department of Nuclear Medicine, FUESMEN, Mendoza, Argentina.
1Chief of Nuclear Medicine Service, Department of Nuclear Medicine, FUESMEN, Mendoza, Argentina.
2Tomography Department, FUESMEN, Mendoza, Argentina.
*Corresponding Author : Ronchi Brunela
Department of Nuclear Medicine, FUESMEN, Mendoza, Argentina.
Email: brunelaronchi@gmail.com
Received : Dec 20, 2022
Accepted : Dec 28, 2022
Published : Jan 04, 2023
Archived : www.jcimcr.org
Copyright : © Brunela R (2023).
Abstract
The superior mesenteric artery syndrome is an uncommon entity included in the spectrum of vascular syndromes. The low presentation, variety of in specific symptoms and shortage of bibliography presents a challenging diagnosis for both clinicians and radiologists. Our aim is to present a 63 years-old male patient with pancreatitis history and repeated symptoms. Further investigation with contrast-enhanced upper abdominal computed tomography revealed the duodenal stenosis and confirmed the diagnosis. Imaging is paramount to exclude differential diagnosis and confirm the superior mesenteric artery síndrome.
Citation: Marinova L, Georgiev R, Evgeniev N. Clinical observations in three clinical cases with locally advanced chordomas. What is needed for early diagnosis with improved survival?. J Clin Images Med Case Rep. 2020; 1(1): 1005.
Case report
A 63 male patient with a history of acute pancreatitis, began 7 months later with epigastric pain, vomiting and considerable weight loss. A non contrast CT scan was performed dismissing post pancreatitis complications. Therefore, as the patient continued symptomatic, a more meticulous examination of the images was done with contrast-enhanced upper abdominal computed tomography.
Imaging findings
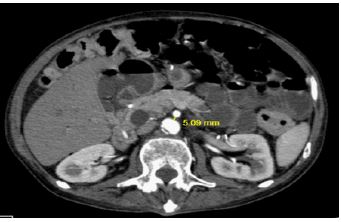
The tomographic scan of the patient shows, in a proximal level, a dilatation of the distal portion of the esophagus visible with liquid level and subsequently, duodenal stenosis in its 3rd portion due to aorto-mesenteric compression. It also presents intramural air from the colonic gastrointestinal tract and from the last ileal loops in relation to intestinal pneumatosis.
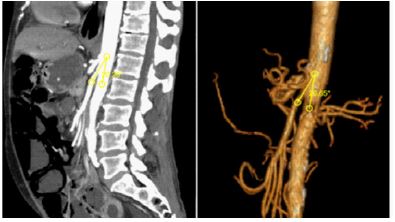
Computed tomography with EV contrast and 3D reconstruction confirms the suspected diagnosis of Wilkie syndrome.
Discussion
Wilkie’s syndrome or superior mesenteric artery syndrome is an unusual and unexpected entity in which there is an obstruction of the small intestine between the Abdominal Aorta (AA) and the Superior Mesenteric Artery (SMA).
As there are only limited cases in the literature and the incidence is unknown, we believe it is important to present this case to highlight this disease and review the literature to consider one of the pathologies of the spectrum of vascular syndromes as causes, also, of nonspecific abdominal pain.
The resultant obstruction may be intermittent, partial or complete, acute or chronic. Among the most frequent symptoms in acute presentation postprandial abdominal pain, weight loss, bloating, eructation, refux, nausea and vomiting have been described [1,5]. All of them due to slow gastric emptying caused by duodenal obstruction. What is more, the pain from SMA syndrome is usually localized slightly above and to the left of the umbilicus, and is relieved by firm hand pressure to the area [3]. Chronic patients report a long history of intermittent postprandial abdominal pain, gastrointestinal discomfort, weight loss, nausea, and bilious vomiting [3].
The most common etiologies include congenital or acquired anatomical abnormalities [1,3].
● Conditions associated with loss of perivascular fat: cancer, acquired immunodeficiency syndrome, malabsorption,bariatric surgery , eating disorders, burn injury, tuberculosis.
● Congenital causes: reduction of the aortomesenteric angle due to a low origin of the SMA that displaces the duodenum cranially or insertional variants of the angle of Treitz [4].
● Patients with a history of corrective scoliosis surgery in which the alignment of the spine would produce an increase in tension in the SMA.
Imaging findings
Initially, x-rays findings show gastric or gastroduodenal distention and a paucity of distal bowel gas [5]. Later, tomographic images include compression of the third part of the duodenum with proximal dilatation of the same and the duodenum. Through a deeper review of the literature, we found as normal parameters to be an aortomesenteric angle between 25°-60° and a distance between the Abdominal Aorta (AA) and the SMA of 10 to 20 mm. In sagittal slices, Wilkie syndrome is defined as an aortomesenteric angle less than 22º (Figure 1) and in axial slices an aortomesenteric distance less than 10 mm (Figure 2) [2,5]. CT angiography provides the added benefit of thin (1-mm) slice thickness and multiplanar 3D reconstructions which allow for more precise evaluation of the aorto-mesenteric angle and aortomesenteric distance [5].
| WILKIE'S SYNDROME DIAGNOSTIC CLUES |
|---|
| ● Aorticomesenteric angle: < 22º ● AA-AMS distance: < 10 mm |
Differential diagnoses
Abdominal pain is a symptom that is very present in daily consultations, both in the emergency service and on duty. Thus, the spectrum of differential diagnosis that needs to be considered has to be shortened by an extensive clinical observation and laboratory analysis. It is important for the clinician to have a high index of suspicion of SMA syndrome in the appropriate patient population in order to perform the appropriate radiological testing and ultimately reach the correct diagnosis [5]. The time of presentation also divides urgencies such as mesenteric ischemia, intestinal volvulus and aneurysms from chronic patients. In this second group the literature includes megaduodenum, annular pancreas, inflammatory lesions and duodenal stenosis [1-3].
Treatment
Conservative treatment is performed in most cases through two main options. Firstly, positional changes are widely recommended, like assuming the knee-chest or side-lying position after eating, owing to widen the aorto-mesenteric angle [3]. Secondly, mechanical decompression with a nasogastric tube has proven to relieve the obstruction. If this is ineffective, surgical duodeno-jejunostomyis performed in specific patients carrying major symptoms.
Conclusion
Imaging plays a pivotal role in the diagnosis of this syndrome with high sensitivity. It proves that a detailed examination of a contrast CT scan is sufficient to the diagnosis mixed with proper clinical correlation. Moreover, the detail and subtlety in the visualization of the images allow us to reach the diagnosis of this shortage and, therefore, unusually considered pathology.
References
- Gozzo et al. CT imaging findings of abdominopelvic vascular compression syndromes: What the radiologist needs to know. Insights into Imaging. 2020; 11:48. https://doi.org/10.1186/s13244-020-00852-z
- AlFaqeeh AA, Syed M, Ammar M, et al. Wilkie’s Syndrome as a Rare Cause of Duodenal Obstruction: Perspicacity Is in the Radiological Details. Cureus. 2020; 12: e10467.
- Mathenge N, Osiro S, Rodriguez II, Salib C, Tubbs RS, Loukas M, et al. Superior mesenteric artery syndrome and its associated gastrointestinal implications. Clinical Anatomy. 2013; 27: 1244–1252.
- Sinagra E, Raimondo D, Albano D, et al. Superior mesenteric artery syndrome: clinical, endoscopic, and radiological findings. Gastroenterol Res Pract. 2018:1937416
- Warncke ES, Gursahaney DL, Mascolo M, Dee E. Superior mesenteric artery syndrome: A radiographic review. Abdom Radiol (NY). 2019; 44: 3188-3194.