
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Pulmonary multinodular amyloidosis: A case report
Alejandro Hernández Solís1; Franco Camacho Delgado1; Zxjal Ramírez Patiño2; Fernando Daniel Córdova Del Oso3; Andrea Quintana Martinez1
1Servicio de Neumología y Cirugía de Tórax. Hospital General de México. “Dr. Eduardo Liceaga”. Ciudad de México, México
2Instituto Politécnico Nacional, Escuela Superior de Medicina. Ciudad de México, México.
3Universidad Nacional Autónoma de México, Facultad de Estudios Superiores Iztacal, Estado de México, México.
*Corresponding Author : Andrea Quintana Martínez
Servicio de Neumología y Cirugía de Tórax. Hospital General de México. “Dr. Eduardo Liceaga”. Ciudad de México, México
Phone: 5585507107
Email: andrea.0314@hotmail.com
Received : Dec 10, 2022
Accepted : Dec 29, 2022
Published : Jan 05, 2023
Archived : www.jcimcr.org
Copyright : © Martínez AQ (2023).
Abstract
Nodular pulmonary amyloidosis is rare in our environment with a low incidence. A 77-year-old female patient, who began her illness 20 days before hospital admission with sporadic non-productive cough without attack to the general condition. Computed tomography scan of the chest showed multiple nodular images of heterogeneous density, some of them hyperdense in calcific range, poorly defined borders, patchy in both hemithoraxes with confluence in basal regions. The histopathological study reported areas of amyloid with positive Congo red staining and upon exposure to polarized light, apple green birefringence was observed. Generaly the presentation is asymptomatic, and the diagnosis is incidental, some clinical manifestations may be dyspnea, cough, hemoptysis. It is important to have a high degree of clinical suspicion to make timely diagnosis.
Keywords: Case report; Amyloidosis; Pulmonary multinodular.
Citation: Solís AH, Delgado FC, Patiño ZR, Del Oso FD, Martinez AQ. Pulmonary multinodular amyloidosis: A case report. J Clin Images Med Case Rep. 2023; 4(1): 2229.
Introduction
Amyloidosis comprises a group of disorders characterized by deposition of abnormally folded proteins in tissues. The deposits are formed from soluble globular proteins, which misfold and aggregate into insoluble fibrils, causing progressive organ damage [1].
At the pulmonary level, these deposits envelop the interstitium, affecting gas exchange and presenting progressive interstitial lung disease [2].
In addition to protein production, there is a failure of the elimination mechanisms for this type of misfolded proteins. Amyloid deposits are metabolically inert, but physically interfere with organ structure and function; some prefibrillar oligomers of amyloidogenic proteins have direct cellular toxicity, being an important component of the pathogenesis of the disease [3].
Amyloid deposits can be localized (10%-20%) or systemic (80-90%). At pulmonary level there are 4 clinical forms: diffuse alveolar septal, pulmonary nodule, bronchial tracheobronchial and pleural amyloid [4]. It predominates in the male gender. The most frequent symptoms are fatigue and weight loss; physical findings are not characteristic, being macroglossia one of the most specific signs [5].
In the USA, 1% of patients with chronic inflammatory conditions such as rheumatic disease, familiar mediterranean fever will develop secondary amyloidosis, while the incidence of primary amyloidosis is 4.5 per 100,000 inhabitants. In Mexico, pulmonary amyloidosis is rare and its incidence is unknown.
Case report
A 77-year-old female patient, who began her illness 20 days before hospital admission with sporadic non-productive cough without attack to the general condition, and she went for medical evaluation. Physical examination revealed pulmonary consolidation syndrome in the right hemithorax.
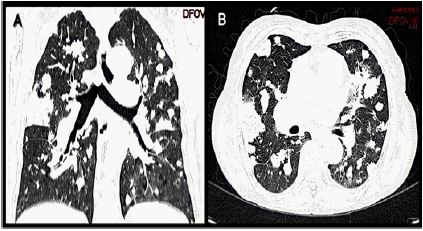
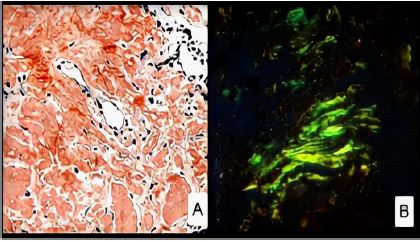
A Computed Tomography (CT) scan of the chest showed multiple nodular images of heterogeneous density, some of them hyperdense in calcific range, poorly defined borders, patchy in both hemithoraxes with confluence in basal regions (Figure 1). A lung biopsy was performed by posterolateral thoracotomy. The histopathological study reported areas of amyloid with positive Congo red staining and upon exposure to polarized light, apple green birefringence was observed (Figure 2).
Laboratory results showed serum kappa levels of 3.3 mg/dl, lambda 26.3 mg/dl, kappa/lambda ratio of 0.125, respiratory function tests reported severe restrictive pattern with a vital capacity of 40%. In our patient there was no evidence of systemic amyloidosis.
Discussion
Nodular pulmonary amyloidosis is rare in our environment with a low incidence, frequent in men aged 50-60 years, with a 3:2 rating and a history of chronic inflammatory conditions such as rheumatic disease, Sjögren’s syndrome, MALT lymphoma or multiple myeloma [6].
At pulmonary level it shows isolated lesions that can be confused with malignant processes. It usually presents as interstitial disease of tracheobronchial location, due to diffuse amyloid deposition in the alveolar septa with a reticular pattern on chest X-ray. Rarely, intraparenchymal lesions appear in a multinodular form, as in the present case.
Generally, the presentation is asymptomatic, and the diagnosis is incidental, some clinical manifestations may be dyspnea, cough, hemoptysis [7]. In the chest X-ray peripheral nodules can be found that can be bilateral of variable size with cystic changes of slow growth. Contrast computed axial tomography is an ideal technique to establish the characteristics and location of the pulmonary nodule. In our case, chest CT showed multiple nodules in both hemithoraxes, with confluence in basal regions. Bronchoscopy is of little use in the diagnosis of peripherally located pulmonary nodules, although it can help in central lesions. Radiologically guided percutaneous fine needle puncture of a peripheral pulmonary nodule has high diagnostic capability and lower risk than a tracheobronchial puncture [8]. To establish a diagnosis of certainty it is essential that a biopsy be stained with Congo red and show apple-green birefringence in polarized light. Histopathological studies reveal eosinophilic density and aggregates of plasma cells and lymphocytes [9].
Systemic presentation requires chemotherapy treatment or autologous stem cell transplantation; treatment for localized forms is symptom oriented. Nodular localized amyloidosis usually progresses and shows recurrence after resection, there is no specific treatment [4,9]. Patients with nodular pulmonary amyloidosis have a good prognosis with timely diagnosis, unfortunately amyloidosis with myeloma has a poor prognosis, with a median life expectancy of 12 to 15 months after diagnosis.
The case presented is relevant for being female, absence of specific clinical data and no history of chronic inflammatory disease, presenting a benign evolution and adequate survival.
Declarations
Acknowledgements: The authors would like to thank the medical and nursing staff of the cardio-pneumology tower of the Hospital General de Mexico “Dr. Eduardo Liceaga”.
Statement of ethics: Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Ethical review board: The authors declare that they have followed the protocols of their work center on the publication patient data.
Right to privacy and informed consent: The authors have obtained the written informed consent from the patient for publication of this case report and any accompanying images. The author is in possession of this document.
Conflict of interest: The authors have no conflicts of interest to declare.
Funding: The authors declare have no commercial or financial relationship with any sponsor, or direct professional relationship with it.
Author contributions: All authors contributed to the preparation and revision of the manuscript.
References
- Picken MM. The Pathology of Amyloidosis in Classification: A Review. Acta Haematol. 2020; 143: 322-334.
- Milani P, Basset M, Russo F, Foli A, Palladini G, Merlini G. The lung in amyloidosis. Eur Respir Rev. 2017; 26: 170046.
- Hazenberg BP. Amyloidosis: A clinical overview. Rheum Dis Clin North Am. 2013; 39: 323-345.
- Zimna K, Sobiecka M, Langfort R, Błasińska K, Tomkowski WZ, et al. Pulmonary amyloidosis mimicking interstitial lung disease and malignancy - A case series with a review of a pulmonary patterns. Respir Med Case Rep. 2021; 33: 101427.
- Cibeira MT, Bladé J. Amiloidosis primaria: diagnóstico, pronóstico y tratamiento. Hospital Clínic. Barcelona.
- Khoor A, Colby TV. Amyloidosis of the Lung. Arch Pathol Lab Med. 2017; 141: 247-254.
- García-Sánchez A, Villasante C, Esteban-Rodriguez I, García-Río FF. Amyloidosis as a Cause of Cystic Pulmonary Fibrosis Associated With Pulmonary Nodules. Arch Bronconeumol (Engl Ed). 2018; 54: 481-482. English, Spanish.
- Guasch M, Ojanguren A, Gómez JR. Pulmonary amyloidosis: A diagnosticchallenge. Cir Esp (Engl Ed). English, Spanish. 2020; 98: 50-52.
- Uzer F, Dirol H. An incidental case of pulmonary Amyloidosis. Int J Respir Pulm Med. 2018; 5: 1-3.