Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Achalasia in the emergency room: An infrequent disease with typical images
Hugo Inácio1*; Leonor Soares2; Rita Lencastre Monteiro1; Ana Catarina Rodrigues3; Diana Carvalho4
1Medicina Interna - Hospital de Santo António dos Capuchos, Centro Hospitalar Universitário de Lisboa Central.
2Medicina Interna - Hospital de São José, Centro Hospitalar Universitário de Lisboa Central.
3Medicina Interna - Hospital Curry Cabral, Centro Hospitalar Universitário de Lisboa Central.
4Gastrenterologia - Hospital de Santo António dos Capuchos, Centro Hospitalar Universitário de Lisboa Central.
*Corresponding Author : Hugo Inácio
Medicina Interna - Hospital de Santo António dos Capuchos, Centro Hospitalar Universitário de Lisboa Central, Portugal.
Phone: +351 964650329;
Email: hinacio@gmail.com
Received : Dec 08, 2022
Accepted : Dec 30, 2022
Published : Jan 06, 2023
Archived : www.jcimcr.org
Copyright : © Inácio H (2023).
Keywords: Achalasia; Acute dysphagia; Megaesophagus; Emergency room.
Citation: Inácio H, Soares L, Monteiro RL, Rodrigues AC, Carvalho D. Achalasia in the emergency room: An infrequent disease with typical images. J Clin Images Med Case Rep. 2023; 4(1): 2232.
Background
A 36-year-old male with no medical history was referred to the Emergency Room (ER) with complaints of vomiting and progressive dysphagia for solids and liquids over a two-week period. The patient denied other symptoms.
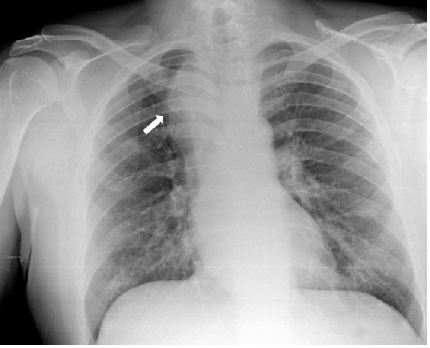
Upon presentation to the ER, both the physical examination and the blood analysis were unremarkable, but the chest X-ray revealed widening of the upper third of the mediastinum (Figure 1). For clarification, a chest Computed Tomography (CT) scan was performed. It revealed diffuse esophageal dilatation (mega esophagus) with thinning at the esophagogastric junction with significant stasis, without abnormal focal parietal thickening (Figures 2 and 3).
In order to drain the esophageal content, a nasogastric tube was placed. An upper gastrointestinal endoscopy confirmed esophageal dilatation and revealed hyperemia and congestion of the distal esophageal mucosa, but the biopsies found no evidence of neoplasia. No lesions were found in the stomach. Conventional esophageal manometry was then performed and the result confirmed the suspicion of achalasia.
This case illustrates the importance of proper diagnosis and treatment of achalasia, as it may cause symptoms such as dysphagia, regurgitation, chest pain, and weight loss, as well as increased risk of esophageal cancer, due to stasis of ingested food.