
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 4
Heterotopic hip ossification in patients with severe acquired brain injury: When surgical intervention is recommended
Lucca Lucia Francesca1; Carallo Orazio Francesco Antonio1; Raso Maria Girolama1; Tonin Paolo1; Cerasa Antonio1,2,3*
1S’Anna Institute, 88900 Crotone, Italy.
2Institute for Biomedical Research and Innovation (IRIB), National Research Council of Italy (CNR), Italy.
3Pharmacotechnology Documentation and Transfer Unit, Preclinical and Translational Pharmacology, Department of Pharmacy, Health Science and Nutrition, University of Calabria, 87036 Arcavacata, Italy.
*Corresponding Author : Antonio Cerasa
Antonio IRIB-CNR, Messina, Italy.
Email: Antonio.cerasa76@gmail.com
Received : Dec 09, 2022
Accepted : Jan 03, 2023
Published : Jan 10, 2023
Archived : www.jcimcr.org
Copyright : © Cerasa A (2023).
Keywords: Severe acquired brain injury; Heterotopic hip ossification; CT 3D.
Citation: Lucca LF, Corallo OFA, Raso MG, Tonin P, Cerasa A. Heterotopic hip ossifications in patients with severe acquired brain injury: When surgical intervention is recommended. J Clin Images Med Case Rep. 2023; 4(1): 2236.
Introduction
The production of ectopic lamellar bone in soft tissues is known as Heterotopic Ossification (HO). HO is a common consequence following trauma, burns, brain injuries, and major orthopedic surgery. It can be thought of as abnormal tissue repair [1,2].
The hip is the joint most frequently affected after a severe acquired brain injury, affecting the prognosis of patients both for those who continue to have persistent disturbances of consciousness, making it difficult for nurses to perform for example hygiene, and for those who regain consciousness but they are limited in their ability to care for their lower body and change posture (for example, from bed to standing). In 2012, Mavrogenis et al [3] presented a new categorization of heterotopic hip ossifications based on axial tomographic pictures considering the limitations of Brooker’s classification [4], which is based on anteroposterior radiography images.
Depending on where heterotopic bone formation around the hip joint occurs, the Mavrogenis classification separates four types of neurogenic HO: 1) type 1 at the anterior hip or the proximal end of the femur, with or without ankylosis; 2) type 2 at the posterior hip or the proximal end of the femur, with or without ankylosis; 3) type 3 at the anterior and medial hip or the proximal end of the femur, with or without ankylosis; 4) type 4 around the hip (circumferential), with or without ankylosis), and 2 subtypes (a and b) according to the etiology of the neurological injury (a: Spinal cord injury; b: Brain injury). According to the anatomical position, this classification allows for preoperative planning of the surgical approach [3].
Here, we presented the relative prognosis of two case reports of non-traumatic ABI patients with HO.
Case 1
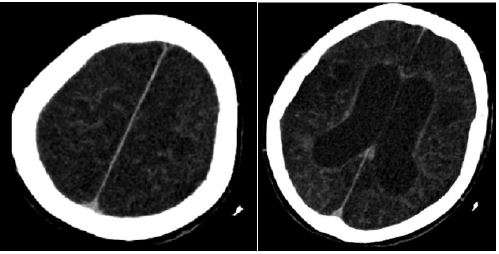
A 61-year-old female with headache and loss of consciousness in 03/31/2020 was immediately brought to the emergency facility where CT and angio-CT scan of the brain revealed rupture of anterior communicating artery aneurysm. The Glasgow Coma Scale was 5 upon admission. On the same day she underwent embolization of the aneurysm and implantation of an external ventricular shunt.
Long-term mechanical ventilation was necessary for the patient. She had a tracheostomy on April 11, 2020, while the external ventricular shunt system was removed on April 20, 2020. She was sent to rehabilitation facility after 30 days from event. She was minimally conscious state when she was admitted, Coma Recovery Scale-revised: 9, Level Cognitive Functioning III; Disability Rating Scale: 22. Radiography of the hips excluded heterotopic ossifications. After initial improvement in cognitive functioning, the patient presented neurological regression. CT scan revealed hydrocephalus and she was sent to neurosurgery unit for peritoneal ventricle shunt implant. Upon returning to the rehabilitation unit, in the face of cognitive improvement, the patient presented pain and limitation of hip joint function, left greater than right.
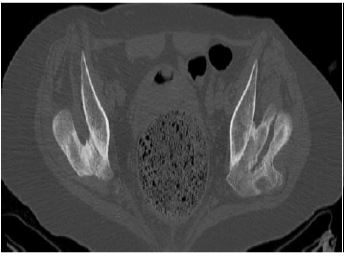
She was discharged home on September 29, 2020, emerged from minimally conscious state, with frontal cognitive deficits, psycho-motor slowness, without tracheostomy tube, with recovery of oral swallowing. The severe disability caused in part by the HO hips for which excision surgery was strongly recommended to be scheduled as soon as possible (Figure 1).
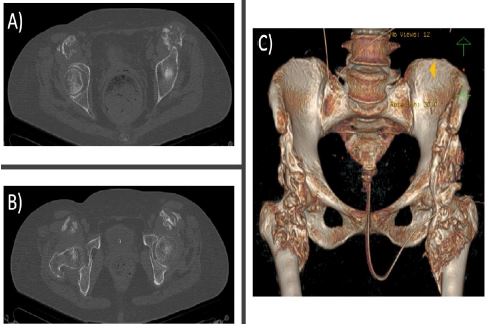
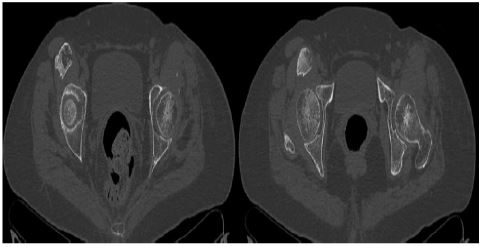
Based on health care access restrictions due to the COVID-19 pandemic, the patient underwent removal of heterotopic ossification of the left hip 15 months after being discharged from the rehabilitation unit. After surgery the patient returned to the rehabilitation unit where a new CT examination was performed (Figures 2,3). Subsequent time spent in a rehabilitation setting led to a return to independence in rising from a seated position and walking with a walker, as well as a reduction in the level of assistance with lower body care.
Surgical resection for nongenetic HO is ideally performed after the osseous maturation is complete, which is typically by 6 months after the initiation of HO. Excision before 6 months HO may be associated with an increased risk of recurrence of HO [5].
Case 2
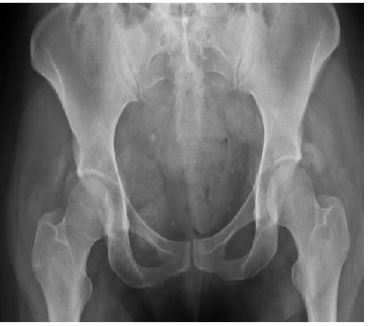
38-year-old female in May 2014 presented post-anoxic coma from cardiac arrest. June 2014 hospitalization in rehabilitation setting: Patient in unresponsive wakefulness syndrome/vegetative state, breathing with oxygen support via tracheostomy, feeding via nasogastric tube, indwelling bladder catheter. Coma Recovey Scale-r 3, Level Cognitive Functioning II; Disability Rating Scale 24. Radiography of the hips 40 days after the event showed initial signs of heterotopic ossifications (Figure 4).
During her stay in rehabilitation the patient with persistent severe disorder of consciousness underwent PEG implant and baclofen pump implant for severe diffuse spasticity.
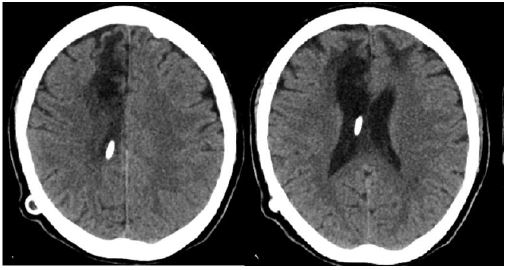
One year after the ABI event, a second expert opinion was in line with the diagnosis of unresponsive wakefulness syndrome/vegetative state. PET-FDG, fMRI, DTI-MRI and hd-EEG confirm the diagnosis (Figure 5). In view of the fact that this condition was considered irreversible, at 18 month after the severe acquired brain injury post-anoxic, the orthopedic specialist considered HO excision surgery not indicated.
CT images and 3D reconstruction (figures 6 and 7) show evolution of hip HO after 8 years.

Discussion
These two case reports of patients with severe acquired vascular brain injury are paradigmatic of different therapeutic approaches based on recovery course of disease. In the first case, despite being less young, the improvement of cognitive functioning, the removal of the trachestomy tube, the recovery of oral nutrition, but also the site of Type 1b HO with a lower risk of bleeding, allowed us to indicate the removal of the HO. After surgery, the patient obtained an improvement in functional level. On the other hand, the neurological status of the second patient, the need for devices such as the tracheostomy and PEG, the risk of greater bleeding given the arrangement of the ossification, led the orthopedic specialist not to give any indication for its removal.
Conclusion
The decision to plan hip HO excision surgery is based on the expected benefit-risk ratio and the patient’s potential for recovery. Patients who remain in conditions of unresponsive wakefulness syndrome/vegetative state in many cases are not candidates for HO removal.
References
- Kaplan FS, Glaser DL, Hebela N, Shore EM. Heterotopic ossification. J Am Acad Orthop Surg. 2004; 12: 116-125.
- Vanden Bossche L, Vanderstraeten G. Heterotopic ossification: A review. J Rehabil Med. 2005; 37: 129-136.
- Mavrogenis AF, Guerra G, Staals EL, Bianchi G, Ruggieri P. A classification method for neurogenic heterotopic ossification of the hip. J Orthopaed Traumatol. 2012; 13: 69–78.
- Brooker AF, Bowerman JW, Robinson RA, Riley LH Jr. Ectopic ossification following total hip replacement: Incidence and a method of classification. J Bone Joint Surg Am. 1973; 55: 1629– 1632.
- Pavey GJ, Polfer EM, Nappo KE, Tintle SM, Forsberg JA, Potter BK, et al. What risk factors predict recurrence of heterotopic ossificatio after excision in combat-related amputations? Clin Orthop Relat Res. 2015; 473: 2814–2824.