
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Life-threatening event after injection laryngoplasty in a patient with chemotherapy-induced vocal-fold motion impairment: A case report
Seung Yeon Jeon1; Soo Jung Gong2; Ra Gyoung Yoon3; Ah Ra Jung1*
1Department of Otorhinolaryngology-Head and Neck Surgery, Nowon Eulji Medical Center, Eulji University School of Medicine, Seoul, Republic of Korea.
2Department of Internal Medicine, Nowon Eulji Medical Center, Eulji University School of Medicine, Seoul, Republic of Korea.
3Department of Radiology, Nowon Eulji Medical Center, Eulji University School of Medicine, Seoul, Republic of Korea
*Corresponding Author : Ah Ra Jung
Department of Otorhinolaryngology-Head and Neck Surgery, Nowon Eulji Medical Center, Eulji University School of Medicine, Seoul, Republic of Korea.
Tel: +82-2-970-8276, Fax: +82-2-970-8265;
Email: jungara2030@eulji.ac.kr
Received : Dec 09, 2022
Accepted : Jan 05, 2023
Published : Jan 12, 2023
Archived : www.jcimcr.org
Copyright : © Jung AR (2023).
Abstract
Background: Although chemotherapy-induced vocal-fold motion impairment was first reported in 1971, there are few reports. Herein, we describe a case in which life-threatening side effects occurred after injection laryngoplasty for the treatment of chemotherapy-induced vocal-fold motion impairment accompanied by dysphonia and aspiration in a patient with lymphoma.
Case presentation: An 86-year-old woman with diffuse large B-cell lymphoma developed left vocal fold immobility with dysphonia and aspiration after six cycles of Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, And Prednisone (R-CHOP) therapy. The patient underwent injection laryngoplasty to prevent aspiration pneumonia approximately 5 h after the 7th cycle of chemotherapy. On the 3rd day after the procedure, she visited the emergency room with swelling of the anterior neck and dyspnea with stridor, which had gradually worsened since the previous day, and emergency hematoma removal was performed. On the 14th day after injection laryngoplasty, laryngeal examination performed to observe the vocal cord bruises revealed improvement of edema. Dyspnea and dysphonia observed before emergency surgery resolved completely one month after the operation.
Conclusions: It is important to promptly evaluate patients with symptoms such as dyspnea and stridor after injection laryngoplasty and select a safe procedure time for patients receiving chemotherapy to avoid serious complications, such as hematomas.
Keywords: Chemotherapy-induced vocal-fold motion impairment; Injection laryngoplasty; Hematoma; Thrombocytopenia.
Abbreviation: CIVFMI: Chemotherapy induced vocal ford motion impairment; DLBCL: Diffuse large B-cell lymphoma; IL: Injection laryngoplasty.
Citation: Jeon SY, Gong SJ, Yoon RG, Jung AR. Life-threatening event after injection laryngoplasty in a patient with chemotherapy-induced vocal-fold motion impairment: A case report. J Clin Images Med Case Rep. 2023; 4(1): 2239.
Background
Diffuse Large B-Cell Lymphoma (DLBCL) is the most common lymphoma, and accounts for 25% of non-Hodgkin lymphoid neoplasms [1]. The addition of rituximab to cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) is currently the standard treatment for patients with DLBCL [2]. Chemotherapeutic agents, such as vinca alkaloids including vinblastine, vinorelbine, eribulin and vincristine, often induce toxic changes, such as neuropathy, in the peripheral nervous system [4]. Although Chemotherapy-Induced Vocal-Fold Motion Impairment (CIVFMI) was first reported in 1971, there are few reports of CIVFMI [5]. In most cases, CIVFMI resolved spontaneously after the cessation of chemotherapy, and the duration of symptoms ranged from 7 to 420 days, with a mean of 105.9 days [5].
Injection Laryngoplasty (IL) using short acting injectable materials is a well-established procedure for the treatment of glottic insufficiency from laryngeal pathology, including vocal fold immobility, unilateral vocal fold paralysis, and presbylaryngis [6]. Hyaluronic acid, which is a naturally occurring polysaccharide in the extracellular matrix of human cells, has also been identified within the lamina propriaof the vocal cords [7,8]. ILs has advantages such as avoiding open surgical procedures and low complication and morbidity rates and can be performed under local anesthesia [9].
Herein, we describe a case in which life-threatening side effects occurred after IL for the treatment of CIVFMI accompanied by dysphonia and aspiration in a patient with DLBCL receiving R-CHOP treatment. Furthermore, we reviewed the literature regarding the timing of IL after CIVFMI to prevent potentially serious adverse effects of therapy in patients with lymphoma.
Case presentation
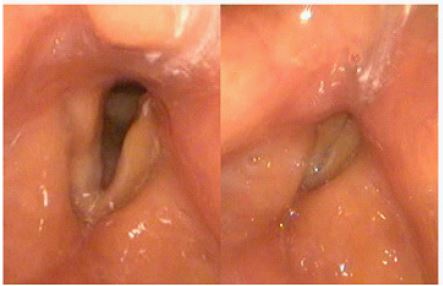
An 86-year-old woman was diagnosed with diffuse large B-cell lymphoma, and started on the R-CHOP regimen on December 11, 2020. On June 30, 2021, she was referred to the department of otolaryngology with complaints of dysphonia and dysphagia that occurred after the 6th cycle of R-CHOP. Flexible laryngoscopy revealed left vocal fold immobility. The left vocal fold was paramedian in position with an approximately 2 mm glottic gap (Figure 1). Laboratory examination showed serum hemoglobin, leukocyte, and platelet levels within normal ranges. She complained of dysphonia, dysphagia, and a high frequency of aspiration during meals; therefore, to prevent aspiration pneumonia, we planned IL on July 21, 2021, when she was scheduled to be admitted to the day-care center for the 7th cycle of R-CHOP. The patient was admitted to the hospital, received chemotherapy with R-CHOP, and approximately 5 h later, IL was performed. After percutaneous local anesthesia of the cricothyroid membrane, 0.6 mL (20 mg/mL) of small-particle stabilized hyaluronic acid (Restylane; Q-Med AB, Uppsala, Sweden), was injected into the left vocal fold (Figure 2). Postoperatively, the patient was discharged after her vital signs stabilized.
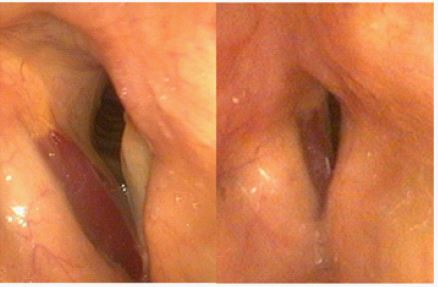
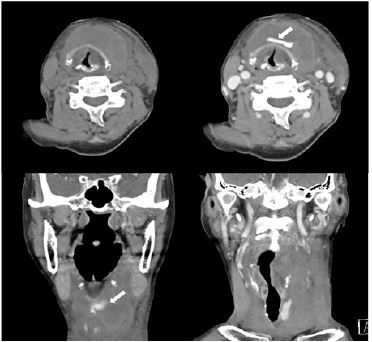
Three days after IL, the patient visited the emergency room with anterior neck swelling and dyspnea with stridor that began on the second postoperative day and gradually worsened. Fiberoptic laryngoscopic examination showed bruising and edema of the right vocal fold (Figure 3). Hematological examination revealed thrombocytopenia with a platelet count of 43,000 /mcL. Moreover, contrast-enhanced computerized tomography demonstrated acute hematoma with extravasation of contrast agent suggesting active bleeding in the visceral space to the left anterior cervical triangle. In addition, diffuse swelling with infiltration of the bilateral paraglottic space, left anterior cervical triangle, and left lateral neck was noted (Figure 4). The patient was promptly referred to the operating room, and emergency neck exploration under general anesthesia was performed. There was no active bleeding focus, but oozing of blood oozed was observed between the cricothyroid membrane and the bilateral strap muscles. The hematoma was removed, and bleeding was controlled using bipolar and absorbable hemostatic products. We did not perform tracheas to my and completed the operation by inserting ahemovac on both sides of the neck. The patient was observed in the intensive care unit for two days while receiving blood transfusions and filgrastim, a hematopoietic agent for thrombocytopenia control, and was then transferred to the general ward. On the 14th day after IL, laryngoscopic examination to observe her vocal cord bruises revealed improvement of edem. The dyspnea and dysphonia observed before emergency surgery resolved completely within one month postoperatively. Three months after IL, the glottic gap was < 2 mm without aspiration or dysphonia (Figure 5). The patient died of lymphoma on December 26, 2021.


Discussion and conclusions
In patients undergoing chemotherapy, motor neuropathy is relatively uncommon compared to sensory neuropathy, and often results from mitotic arrest and subsequent cell apoptosis [3]. CIVFMI is an uncommon complication, with few reports of neurotoxic effects of anticancer agents, such as peripheral neuropathy [4]. Although adverse effects resolve spontaneously after the cessation of chemotherapy in most cases, CIVFMI can present with a variety of aerodigestive symptoms, including dysphagia, dysphonia, and dyspnea [5]. These symptoms are not specific to CIVFMI, but are similar to those associated with vocal-fold motion impairment.
IL improves glottic insufficiency through medialization of the vocal folds and can be performed under local anesthesia in an awake-patient. Hyaluronic acid is the most commonly used agent owing to its ease of use and low complication and high improvement rates [10]. However, serious life-threatening reactions have been reported following IL. Between 2009 and 2020, 47 individual adverse events were reported after IL, and the most common adverse reactions were laryngeal edema (39.1%), persistent dysphonia (28.3%), and dysphagia or dysphagia after injection (23.9%) [11]. Of the 47 reported adverse events, 29 (63%) were major complications (defined as requiring emergency room treatment, hospitalization, intubation or tracheostomy, and surgical intervention), including postoperative airway obstruction due to hypersensitivity [11]. Halderman et al. reported one life-threatening postoperative hematoma with dyspnea and voice changes after 82 injections in 64 patients [6].
To the best of our knowledge, a hematoma caused by IL in a patient with CIVFMI has not been reported previously. Our patient presented with unilateral CIVFMI with dysphonia and aspiration that was diagnosed as DLBCL and developed after six cycles of the R-CHOP regimen. To prevent aspiration pneumonia, which is highly fatal in patients undergoing chemotherapy, we planned IL. The patient received the 7th cycle of R-CHOP, and approximately 5 h later, IL was performed according to the classical procedure. There were no specific findings during the procedure. After the procedure, the patient’s vital signs were stable, and she was discharged. Three days after IL, a life-threatening hematoma with thrombocytopenia with a platelet count of 43,000/ mcL developed, and emergency surgery was performed.
To the best of our knowledge, there are no reports of IL in patients undergoing chemotherapy, and there is no literature on the timing of IL. The frequency of thrombocytopenia differs depending on the regimen used, and is 5-9% with R-CHOP [12]. Thrombocytopenia caused by chemotherapy can cause complications after major surgery as well as simple procedures such as IL. The onset of thrombocytopenia is generally between 7 and 10 days, and it can persist for 30-60 days [12]. The appropriate time interval between chemotherapy and surgery has not been described well in previous studies; however, surgery should be performed when the neutropenic window has passed, which is generally between 3 and 4 weeks [13].
In conclusion, this case highlights that dysphonia and aspiration may be signs of CIVFMI. Early identification of CIVFMI and appropriate surgical intervention are essential for managing this disorder. IL avoids open surgical procedures such as tracheostomy, has fewer complications, and improves the quality of life in patients with CIVFMI. However, it is important to promptly evaluate patients with symptoms such as dyspnea and stridor after IL and select a safe procedure time for patients receiving chemotherapy to avoid serious complications such as hematomas.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Consent for publication was obtained from the patient according to our institutional consent form.
Availability of data and materials: The data that support the findings of this study are available from the Nowon Eulji Medical Center. Data are available from the authors upon reasonable request and with the permission from the Now on Eulji Medical Center.
Competing interests: The authors declare that they have no competing interests.
Funding: Not applicable.
Author’s contributions: SYJ and ARJ designed the study and drafted the first manuscript. RGY performed the radiological diagnosis and evaluated the images. RGY, SJG, and ARJ reviewed the manuscript drafts and provided critical revisions. All authors have read the final manuscript and approved this submission.
Acknowledgements: This research was supported by EMBRI Grants 2020-07-031 from the Eulji University.
References
- Teras LR, DeSantis CE, Cerhan JR, Morton LM, Jemal A, et al. US lymphoid malignancy statistics by World Health Organization subtypes. CA: A cancer journal for clinicians. 2016; 66: 443-459.
- Coiffier B, Thieblemont C, Van Den Neste E, Lepeu G, Plantier I, et al. Long-term outcome of patients in the LNH-98.5 trial, the first randomized study comparing rituximab-CHOP to standard CHOP chemotherapy in DLBCL patients: A study by the Groupe d’Etudes des Lymphomes de l’Adulte. Blood, The Journal of the American Society of Hematology. 2010; 116: 2040-2045.
- Grisold W, Cavaletti G, Windebank AJ. Peripheral neuropathies from chemotherapeutics and targeted agents: diagnosis, treatment, and prevention. Neuro Oncol. 2012; 14: iv45-iv54.
- Brook J, Schreiber W. Vocal Cord Paralysis: A Toxic Reaction to Vinblastine (NSC-49842) Therapy 1, 2, 3. Cancer Chemotherapy Reports. 1971; 55: 591-593.
- Talmor G, Nguyen B, Geller MT, Hsu J, Kaye R, et al. Vocal Fold Motion Impairment Following Chemotherapy Administration: Case Reports and Review of the Literature. Ann Otol Rhinol Laryngol. 2021; 130: 405-415.
- Halderman AA, Bryson PC, Benninger MS, Chota R. Safety and length of benefit of restylane for office-based injection medialization-A retrospective review of one institution’s experience. J Voice. 2014; 28: 631-635.
- Prendes BL, Yung KC, Likhterov I, Schneider SL, Al‐Jurf SA, et al. Long‐term effects of injection laryngoplasty with a temporary agent on voice quality and vocal fold position. The Laryngoscope. 2012; 122: 2227-2233.
- Hertegård S, Dahlqvist Å, Laurent C, Borzacchiello A, Ambrosio L, et al. Viscoelastic properties of rabbit vocal folds after augmentation. Otolaryngology–Head and Neck Surgery. 2003; 128: 401-406.
- Kwon TK, Buckmire R. Injection laryngoplasty for management of unilateral vocal fold paralysis. Current opinion in otolaryngology & head and neck surgery. 2004; 12: 538-542.
- Song PC, Sung CK, Franco RA, Jr. Voice outcomes after endoscopic injection laryngoplasty with hyaluronic acid stabilized gel. Laryngoscope. 2010; 120: S199.
- Din-Lovinescu C, Talmor G, Gravina A, Kaye R, Mansukhani P, et al. Adverse events following injection laryngoplasty: An analysis of the MAUDE database. American Journal of Otolaryngology. 2021; 42: 103092.
- Kuter DJ. Managing thrombocytopenia associated with cancer chemotherapy. Oncology (Williston Park). 2015; 29: 282-294.
- Yoo TK, Moon HG, Han W, Noh DY. Time interval of neoadjuvant chemotherapy to surgery in breast cancer: How long is acceptable? Gland Surg. 2017; 6: 1-3.