
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Review Article - Open Access, Volume 4
Toxic metals and antidotes
*Corresponding Author : Irena kostova
Department of Chemistry, Faculty of Pharmacy, Medical University-Sofia, 2 Dunav St., Sofia 1000, Bulgaria.
Email: irenakostova@yahoo.com
Received : Dec 03, 2022
Accepted : Jan 05, 2023
Published : Jan 12, 2023
Archived : www.jcimcr.org
Copyright : © Kostova I (2023).
Abstract
Heavy metal intoxication is a consequence of the accumulation of metals in the body. The toxicity of heavy metals, particularly lead, arsenic, cadmium and mercury, remains a significant problem and challenge for future investigations. The toxic metals compete with or replace some vital biogenic metals in the course of which some of the biosystems could be affected. One of the most widely used, affordable and simple methods of detoxification is the chelation therapy that causes the toxic element to bind with the drug and be excreted. Many chelating agents, which form stable complexes with heavy metal ions, are commonly used as antidotes in case of heavy metal poisoning. Their effects against metal toxicity are reviewed in the present article. Numerous factors have been revealed to affect the efficiency of the chelation treatment. Most clinically used chelators have also disadvantages including administration in convenience, adverse effects caused by the loss of essential metals, non-specific binding etc. General principles for research and development of new chelators are briefly outlined. Combination of chelating agents and antioxidants is one of the directions of chelation therapy. The search for new chelating agents with specific activity, little side effects and improved therapeutic outcomes is in progress.
Keywords: Lead; Arsenic; Cadmium; Mercury; Chelation therapy; Chelating agents; Oxidative stress.
Citation: Kostova I. Toxic metals and antidotes. J Clin Images Med Case Rep. 2023; 4(1): 2240.
Introduction
Of the objects of bioinorganic chemistry, it is heavy metals in the form of complexes that are most dangerous for the vital activity of organisms. Heavy metals are not metabolized by living systems, which eventually leads to their accumulation to toxic levels [1,2]. The heavy metals attack targets heme-containing proteins and enzymes, systems of peroxide and free radical oxidation of lipids and proteins, antioxidant protection systems, enzymes of electron transport and ATP synthesis, cell membrane proteins and membrane ion channels. The toxic Pb(II), Hg(II), Co(II), Cd(II) ions form strong complexes with amino acids and many other bioligands, especially those containing groups RS- and HS-. Toxic effects of copper compounds are connected with the fact that copper ions interact with thiols -SH groups and amino –NH2 groups blocking proteins. This can be caused by a chelation reaction, as a result of which proteins become insoluble, lose enzyme activity and disrupt vital functions. Toxic effects of silver compounds are associated with the fact that Ag+ interact with toxic S- and N-containing proteins (nucleic acids). Similar is the effect of gold compounds. Toxicity increases with atomic number in the respective series. The toxic effect of heavy metals is manifested in the fact that, having a suitable size and nature of the electron shell, they can integrate into the corresponding receptors instead of biogenic metals, damaging their homeostasis and blocking the action of heavy metals substrates.
Metal-ligand homeostasis is a form of the general homeostatic system. The body has a clear self-regulatory systems homeostasis. The level of the elements in the blood is supported by regulatory mechanisms: absorption processes, separation of water, electrolytes and non-electrolytes, constant stability of chelates. Poor absorption of heavy metals is a consequence of the formation of slightly soluble complexes. Often abnormal digestive processes or alteration cause a violation of homeostasis. There are many ways of metal-ligands regulation of homeostasis.
There are numerous attempts to classify chemical elements according to the degree of interaction with living organisms based on combinations of such parameters as prevalence, availability, digestibility, toxicity. An important role is played by the form of finding an element in the body and its ability to accumulate in a particular organ or tissue. Considering the toxic effects of the environment, the terms “toxic elements” or “toxic compounds” are often used. However, the toxic effect of an element significantly depends on its general and local prevalence in the environment, including whether the toxic compound is natural or was formed as a result of human activity, meaning, it has an anthropogenic nature.
In addition, no compound is completely toxic or completely non-toxic. Each organ or tissue of a living organism functions normally only for a certain interval (permissible values) of concentrations of the respective compound. Deviations in the content of this compound from the norm cause a pathological reaction and is, in fact, the cause of toxicity. The toxicity of the compounds is significantly affected by the dose, the common properties of the compound, the ability of the biological system to absorb and transport the compound to the desired organ, the capability of the compound to transform into more or less toxic forms and its ability to interact with biomacromolecules. Currently, there are special branches of science, such as toxicology, ecotoxicology, which have arisen at the intersection of biology, medicine, physiology, genetics, chemistry, which intensively study the causes of substance toxicity and detoxification methods.
Toxic and non-toxic metals
The necessary elements ensure the maintenance of the dynamic balance of the vital processes of the body. Toxic elements, as well as an excess of necessary elements, can cause irreversible changes in the dynamic equilibrium of biological systems, leading to the development of pathology. The damaging effect of the substance is displayed at various structural levels: molecular, cellular and at the level of the body. The most important abnormal effects occur at the molecular level: inhibition of enzymes, irreversible conformational changes in macromolecules and, as a consequence, changes in the rate of metabolism and synthesis, the occurrence of mutations. Toxic indications depend on the concentration and dose of the substance. Doses can be qualitatively divided into categories according to the degree of effect increase: No noticeable effects; stimulation; therapeutic effect; toxic or damaging effect; death. Stimulation and therapeutic effects may not be caused by all substances.
Toxic metals are chemical elements that have a negative effect on living organisms, which manifests itself only when a certain concentration is reached, determined by the nature of the organism. The most toxic elements are Be, Ba, Tl, As, Sb, Bi, Pb, Se, Te, Cu, Ag, Au, Zn, Cd, Hg, Cr, Ni, Pd, Pt. With the exception of Be and Ba, these elements from stable sulfide compounds. It is believed that the main cause of the toxic effect of these elements is associated with the blocking of certain functional groups (in particular, sulfhydryl proteins) or the displacement of metal ions from certain enzymes, for instance, Cu and Zn. Be, Pb, Cu, Cd, Hg, Cr, Ni, are particularly toxic and prevalent. They compete in the complexation processes with biogenic metals and can displace them from biocomplexes [3,4].
Since many of the metals belong to rare and scattered elements, their toxicity is not so significant. The toxicity of those compounds that are poorly soluble in water (inorganic sulfides) and are not absorbed by the body is also reduced. However, the toxicity of compounds of some elements, for instance, mercury, is increased due to the action of microorganisms that easily absorb poorly soluble mercury compounds and then transfer them to higher animals. Most of the heavy metals are usually toxic because they block many enzymes in the body. Pb (II) ions inhibit acetylcholine esterase, alkaline phosphatase, adenosine triphosphatase, carbonic anhydrase, cytochrome oxidase. Cd (II) ions inhibit adenosine triphosphatase, alcohol dehydrogenase, amylase, carbonic anhydrase, carboxypeptidase, glutamine oxaloacetate transaminase. Hg (II) ions inhibit alkaline phosphatase, glucose-6-phosphatase, lactate dehydrogenase. Additionally, most of the toxic metals are able of form covalent bonds with carbon, resulting in harmful metal-organic compounds.
Lead, arsenic, cadmium and mercury
According to the principle of Hard and Soft Acids and Bases (HSAB), acid-base interactions proceed in such a way that hard acids preferably bind to hard bases, and soft acids to soft bases. Cd2+ and Hg2+, belong to IIB group in the periodic table of elements and are classified as typical soft cations, which prefer coordination with ligands containing soft groups like R2S, RSH, and RS. The coordination of Hg2+ is predominantly linear, whereas in the case of Cd2+ cations, the possibility of forming tetrahedral chelate structures favors their stability. The lead cation Pb2+ (IVA group) is an intermediate ion, signifying that it would coordinates with amino groups, though some interactions with hard O-donor groups and soft S-based groups are detected in many complexes.
Lead
The clinical exhibition of Pb toxicity, known since ancient times, is named “plumbism”. The effects of lead poisoning vary depending on the age of the patient and the amount of exposure. Lead binds to sulfhydryl and amide group constituents of enzymes, changing their configuration and weakening their activities. It also competes with vital metal cations for binding sites, inhibiting enzyme activity, or affecting the transport of essential cations like Ca2+. The disturbance of Ca metabolism is one of the most important mechanisms identified for lead induced neurotoxicity. Lead harmful effects on the hematopoietic system, nervous system, and kidneys have been observed. Oxidative stress has been also implicated as a pathological disorder in lead toxicity [5-7].
Arsenic
Arsenic toxicity is connected with various renal, hepatic, neurological and skin disorders. It also produces carcinogenic effects at chronic exposure however the mechanisms by which as causes human cancers are not yet clear. This element is rapidly and expansively accumulated in the spleen, kidneys, lungs, gastrointestinal tract and mainly in the liver, where inhibits NAD-related oxidation of pyruvate and α-ketoglutarate because of the complexation of As3+ with neighboring thiols. Poison ous effects of as also consist of changes in behavior, confusion, memory loss etc. One of the most important mechanisms of induced disorders by arsenic is its capability to bind with sulfhydryl group (-SH) of biomolecules [8-11].
Cadmium
Cadmium is one of the most toxic metals. Cd2+ ions can be absorbed by most of the body tissues, concentrated mainly in liver and kidney [12]. Having a long biological half-life of almost 20 years in humans, cadmium is recognized as one of the most harmful pollutants [13]. Because its excretion is slow, cadmium accumulation in the body can be significant, especially in the brain tissues. The most hazardous characteristic of Cd is that it accumulates all over the lifetime [14,15]. Chronic exposure to cadmium results in renal, hepatic dysfunction, anemia, osteotoxicity, and cancer in various organs. Cadmium is a strong human carcinogen, associated mainly with lung, prostate, pancreas, and kidney cancers [16]. Cd-induced nephrotoxicity is the most significant and frequent complaint in humans at chronic exposure to cadmium. The toxic effects induced by Cd in biological systems might be attributable to modifications in the antioxidant defense system. Cadmium increases the lipid peroxidation and inhibits enzymes that prevent the oxidative damage. Cd reduces glutathione and protein-bound sulfhydryl groups, resulting in enhanced generation of ROS such as hydrogen peroxide, superoxide ion, and hydroxyl radicals. There is no effective chelation therapy against cadmium intoxication [17].
Mercury
In the environment, living organisms are exposed to several chemical forms of mercury, including elemental Hg vapor, inorganic mercurous Hg (I) and mercuric Hg (II) compounds as well as organomercury compounds. Metallic mercury and inorganic Hg compounds are not considered carcinogenic, whereas organomercury compounds are very dangerous and possibly carcinogenic to humans. Elemental mercury released from dental amalgamsis converted in the body into inorganic mercury which accumulates predominantly in the brain [18]. Metallic mercury vapor is neuro- and nephrotoxic [19,20]. Hg (I) and Hg (II) ions convey their toxicological effects primarily through interactions with sulfhydryl groups on various biomolecules like GSH, metallothionein and albumin, altering protein structures and inhibiting enzymes functions [21]. Additional mechanisms of Hg toxicity have been also suggested including oxidative stress induction, damage of Ca homeostasis, etc. [22].
Detoxification
Maximum toxicity is shown by the most chemically active particles, coordinated unsaturated ions, which include free metal ions. A decrease in the electrophilic properties of the ion, respectively, leads to a decrease in its toxic effect on the body.
One of the most widely used, affordable and simple methods of detoxification is the chemical method. Chemical methods of biotransformation of harmful particles to the body are various, for instance, neutralization of the toxicant by chemical interaction with it (direct effect on the toxicant) and/or elimination of the toxic effect by affecting the enzymes, receptors of the body, which control the physiological processes of utilization of toxicants in the body (indirect effects on the toxicant).
Substances used as detoxifiers allow to change the composition, size, charge sign, properties, solubility of a toxic particle, turn it into a low-toxic one, stop its toxic effect on the body, remove it from the body.
Chelation therapy
Of the chemical methods of detoxification, the most important is the chelation therapy. Harmful substances can be excreted from the body through bioligand that binds to them into complexes. Many chemical elements interacting with bioligands affect positively immunogenetics (protective reaction), increase the formation of antitoxins.
Chelation therapy is widely used, based on the chelation of toxic particles [23,24]. Chelating agents are organic or inorganic compounds capable of binding metal ions to form complex structures, so-called “chelates”. Commonly S, N and O atoms function as ligand donor atoms in the form of chemical functional groups like -NH2, =NH, -SH, -S-S, -OH, -OPO3H, >C=O of biomolecules. The ligands are mainly bidentate or multidentate thus forming stable ring structures. Five-and six-membered chelate rings are particularly stable usually formed by organic ligands with XCCX skeletons such as X-CH2-CH2-X, X-CO-CH2-X etc. where X is O, OR, S, NR, NR2, etc.
Chelating agents provide detoxification of the body by their direct interaction with the toxicant, the formation of a bond, durable form suitable for transportation and excretion from the body. In many cases metal ions form strong bonds with other sulphur-containing ligands which can be used in poisoning as antidotes. One of the most important determining factors is the stability constant of the produced complex which depends on the properties of both the chelated metal and the chelating agent. The readily available in the body fluids Ca2+ ions can bind favorably with chelating agents and compete with Pb2+ ions, for instance. Additionally, pH is also a significant factor influencing the formation and stability of the complex produced. Most of the chelating agents are not stable at low pH. In the simplest case H+ cation that can interact with a lone pair of electrons of the ligand-donor atom/s may be involved in the process of complex formation. On the other side, at high pH the heavy metals have a tendency to form insoluble metal hydroxides and become less reachable to chelating agents especially in some pathological conditions resulting to acidosis or alkalosis. Thus, the expectation of the result is unclear and limited. A chelator action in vitro might not prove so in vivo, which in many cases depends on the presence of endogenous ligands which can also chelate the metal ions competitively. The chelator should have great affinity to the toxic metal to reach the location of metal storage. It should be low toxic and highly soluble in water and in body fluids. The chelating agent must compete with natural chelators and be resistant to biotransformation. Metal complexes formed upon chelation should be less toxic than the free metal ion and easily excreted from the body.
Chelating agents used as antidotes
Many chelating agents, which form stable complexes with heavy metal ions, are commonly used as antidotes in case of heavy metal poisoning. They form soluble complexes which can be eliminated from the body with usual waste products.
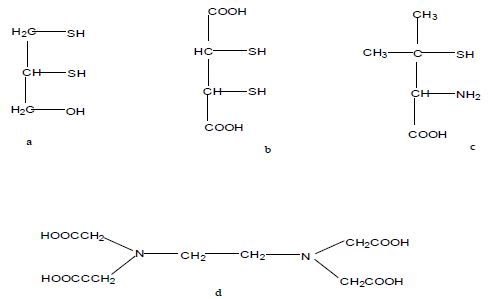
The organic dithiol ligand 2, 3-dimercapto-1-propanol (BAL, dimercaprol, Figure 1a) forms complexes through its two S atoms and facilitates the excretion of the toxic As, Hg, Sb, and Au ions from the body [25]. It contains a 3-carbon backbone with two sulfhydryl (-SH) groups and a hydroxyl group. 2, 3-Dimercaprol has long been the main agent of chelation therapy for Pb or As poisoning, however its serious side effects (substantial increase in brain deposition of toxicants and intramuscular administration) have led to its replacement and the development of less toxic analogues. Even though, due to its high efficiency, it is still prescribed for general metal intoxication for human poisoning with As and Hg compounds. It forms a stable five-membered as complex. This drug is contraindicated in the treatment of Cd and organomercury poisonings.
Dimercaprol has been modified into meso-2, 3-dimercaptosuccinic acid (Succimer, DMSA, Figure 1b), a related dithiol with far less side effects, used in organic Hg intoxication. The hydrophilic nature of this compound causes significant absorption in gastrointestinal tract and consequently its oral administration creates the respective advantages over dimercaprol. Hydrophilic chelators like DMSA effectively promote renal metal elimination, but their capacity to access intracellular metal ions is weak. DMSA is the least toxic among the other dithiol compounds [26]. No significant damage is observed on the amounts of basic metals such as Zn, Ca, Fe and Mg.
Alternative water-soluble dithiol compound, sodium 2,3-dimercaptopropane 1-sulfonate (Unitiol, DMPS), has been introduced as a chelator of Hg poisoning, most often due to amalgam dental fillings. This compound is less effective than CaNa2 EDTA and DMSA and thus not considered a suitable drug against Pb toxicity [27,28]. DMPS is hydrophilic in nature and is distributed mainly in the extracellular spaces. No seriousside effects at DMPS administration have been reported. The metal chelating activity of DMSA is due to the presence of neighboring dithiol groups that can also function as an oxygen radical scavenger and therefore inhibit lipid peroxidation, providing an additional advantage of fighting the oxidative stress induced by heavy metals. However, its use is frequently accompanied by some loss of Cu and Zn.
A large number of mono- and diesters of DMSA have been synthesized which might be more effective antidotes for heavy metal toxicity, compared to DMSA [29]. The controlled esterification made the compounds more lipophilic. Their improved chelating properties are attributed to the higher lipophilicity, favoring cell penetration. It has been observed that these ester derivatives of DMSA were capable of crossing the bio-membranes and were more active in the treatment of arsenic intoxication.
Monoisoamyl DMSA (MiADMSA), obtained by controlled esterification of DMSA with isoamyl alcohol, is lipophilic in nature as compared to DMSA. It shows high efficiency in reducing heavy metal intoxication, especially extracellularly distributed Cd [30]. The toxicity of MiADMSA, similar to that of DMSA, is mediated mainly through the affected copper metabolism [31].
Monomethyl DMSA (MmDMSA) with a straight and branched chain methyl group and monocyclohexyl DMSA (MchDMSA) with a cyclic carbon chain have better lipophilic features and can penetrate cells more readily. Both these agents are orally active and may possess considerable advantages in the clinical treatment of lead toxicity.
It is known that sulfhydryl-based compounds can successfully chelate metals and most of proteins and peptides possess metal-binding sites for detoxification of metal ions. The -Cys-Cys- and -Cys-X-X-Cys- parts of numerous proteins are identified to have binding properties with heavy metal ions. Thus, the S-containing amino acids methionine and cysteine, the metabolite S-adenosyl-Met, α-lipoic acid, the tripeptide Glutathione (GSH) as well as N-acetyl-Cys, all are good chelating agents contributing to the metal excretion from the human body. Cysteine is used in Pb and Cu poisoning [32]. The organo-sulfur compound α-lipoic acid ((R)-5-(1,2-Dithiolan-3-yl) pentanoic acid, LA), essential for aerobic metabolism, is normally produced in the body. Its reduced water-soluble form, dihydrolipoic acid (6,8-bis (sulfanyl) octanoic acid, DHLA), includes a pair of thiol groups. Only the R-enantiomer is therapeutically active in Hg detoxification [33].
The sulfhydryl containing amino acid D-penicillamine (Cuprimine, DPA, β-β-dimethylcysteine or 3-mercapto-D-valine), Figure 1c, is a degradation product of racemicpenicillin. D-Penicillamine is used mainly as an antidotin heavy metal toxicity of lead, mercury and copper (in Wilson’s disease) [34,35]. Only the D-isomer is used.
The synthetic polyamino-polycarboxylic acid Ethylenediaminetetraacetic Acid (EDTA, Figure 1d) and its soluble salts are widely used in poisoning with heavy metals and radioactive isotopes. It has been suggested that EDTA therapy reduces the oxidative stress and inflammation.
Calcium Disodium Salt of Ethylenediaminetetraacetic Acid (CaNa2 EDTA) is the most frequently used chelating agent used for the treatment of lead intoxication. This activity is due to the capability of Pb2+ to displace Ca2+ ions from the chelate. Therefore, CaNa2 EDTA can be effective for the treatment of intoxication by metals which have higher affinity for chelator than does calcium ions. The sodium salt of EDTA, administered in vivo, leads to hypocalcemia due to the calcium complex formation. The lead complex of EDTA is very stable. Extended treatment with CaNa2 EDTA leads to the reduction of vital biogenic metal, particularly Zn, Cu and Mn.
Calcium Trisodium- Diethylenetriaminepentaacetate (CaNa3 DTPA) or Zinc Trisodium-Diethylenetriaminepentaacetate (ZnNa3 DTPA) have been applied against plutonium and other transuranic elements like americium, californium, and curium. The drugs are efficient against Co, Cd and Zn poisoning [36]. CaNa3 DTPA is teratogenic like CaNa2 EDTA due to the reduction of vital Zn and Mn.
Desferrioxamine (Deferoxamine, DFOA) is a trihydroxamic acid, siderophore secreted by fungus Streptomyces pilosus. It is used to remove excess Fe or Al from the body. This chelating agent is identified for its strong binding affinity for Fe3+ and less affinity for other metal ions making it a specific chelator for Fe related diseases for instance thalassemia as well as aluminum poisoning. This drug is well tolerated with few adverse effects [37]. DFOA, being a typical trivalent iron chelator, entirely covers the surface of Fe3+ through complex formation, thus preventing the free radical interactions catalyzed by iron. In contrast, EDTA is not able to protect the Fe3+ ion surface, because it forms a complex with an open structure, which increases the catalytic capability of Fe3+ ions to generate oxidative stress.
Deferiprone (1,2-dimethyl-3-hydroxypyrid-4-one) is an iron chelator and is considered an appropriate alternative to DFOA in the trasfusional Fe overload [38]. Like deferoxamine, deferiprone has also revealed cardioprotective effects. This may be attributed to reduction in Fe overload however, the exact mechanism is not clear [39]. Its major advantages include oral administration, rare side effects and rapid absorption through gastrointestinal tract.
Tetraethylenetetraamine (trientine, TETA) is an antidote for acute copper intoxication. Increased urinary copper excretion has been observed after administration of TETA [40]. Wilson’s disease is characterized by copper homeostasis disturbance which leads to progressive increase in Cu accumulation. Wilson’s disease was originally treated with D-penicillamine but TETA was found to be a better Cu chelator and potentially free of side effects, typical for D-penicillamine [41].
Nitrilotriacetic Acid (NTA, C6H9NO6), is a polyamino-carboxylic acid which is used as a chelating agent for Ca2+, Cu2+ and Fe3+. Its usages are relatively similar to EDTA. Nevertheless, in contrast to EDTA, nitrilotriacetic acid is easily biodegradable. It may be used as a sodium salt (Na3 NTA) and as an iron salt (Fe NTA) in chelating reactions [42]. NTA has been used in the removal of nickel, manganese, zinc and calcium. While Fe NTA causes an iron overload and lipid peroxidation in cells and is genotoxic, the sodium salt Na3 NTA predominantly binds to Zn and Ca, there by exerting its toxic effects.
Thiocarbamates are also effective antidots. Diethyldithiocarbamate (DDC) is an efficient chelator for acute Cd intoxication [43]. As a whole, this compound forms very lipophilic complexes with divalent ions, although enlarged brain deposition has been reported for Hg and Pb, caused by its exposure. Some higher molecular weight DDC derivatives seem promising in mobilizing Cd2+, such as N (methoxybenzyl)-D-glucamine-dithiocarbamate.
Some complexes can also be used to insert some substances into the body, which do not cross the cell membranes in their free form, e.g., Fe3+ ions in the form of a complex with 8-hydroxyquinoline and many other therapeutically active metal complexes.
The most typical structures of important detoxifiers (antidotes) are presented in Figure 1.
Limitations of current chelation therapy
Most of the currently used chelating agents are compromised with many and serious adverse effects. CaNa2EDTA is a main chelating agent for various metal ions but it cannot pass through cellular membranes. In the same way, DMSA shares the restriction of the extracellular distribution. Thus, it is of immediate health concern to identify the limitations of currently available chelating agents and develop new strategies for designing drugs that are more effective in the cases of low, long-term exposure to toxic metals. Although treatment with DMSA and DMPS has shown reduced side effects, essential metal loss particularly of iron, copper and zinc is considered as one of the serious limitations. The specificity of the target metal may be another area to consider when developing new drugs for detoxification of heavy metals.
Combination therapy
A new trend in chelation therapy is the use of two structurally different chelators (combination therapy). The concept of using combined treatment is based on the hypothesis that various chelators are expected to mobilize toxic metals from different tissue locations. Various cases of combined administration have been reported to be beneficial. The combinations of EDTA with BAL and BAL with DMPS have been recommended for long time in inorganic Pb and Hg0 vapor poisonings, respectively. DMSA with CaNa2 EDTA against chronic lead poisoning and DMSA with MiADMSA in reducing arsenic-induced oxidative stress are also good options [44,45]. Since MiADMSA is lipophilic it can bind intracellular toxic metal and make it reachable to extracellularly accessible DMSA thus facilitating fast excretion of metal ions from the body. Additionally, the sulfhydryl groups present in DMSA and MiADMSA may interact with free oxygen radicals and these chelators may act as antioxidants. This combination is proven more efficient than each agent alone in promoting Cd mobilization. Furthermore, it has been shown that combined administration of MiADMSA and CaNa2EDTA is beneficial against chronic lead toxicity. There are observations that DMSA, used in combination with the antibiotic Monensin (sodium salt of monensic acid), is more effective than self-use, specifically in lead removing [46].
Oxidative stress in metal toxicity and the role of antioxidants during chelation
Oxidative stress is considered one of the main mechanisms contributing to heavy metal toxicity, providing a strong basis for the incorporation of antioxidants into chelation therapy. Though the metal induced oxidative stress is recognized, the utility of antioxidants in combination with chelation therapy has not been comprehensively investigated.
Arsenic is one of the most widely studied toxic metals that induces ROS generation and leads to oxidative stress. The exposure to arsenite produces superoxide radical ion and H2O2 in cellular systems. Arsenic is identified not only to produce ROS but also dimethylarsinic peroxyl radical (CH3)2AsOO•, dimethylarsinic radical (CH3)2As•, nitric oxide NO• and hydroxyl •OH radicals [47].
Oxidative stress is also involved in Hg-induced toxicity. This metal reduces the function of the main intracellular antioxidant GSH. Cadmium, contrasting other heavy metals, is unable to generate free radicals by itself, but produces superoxide radical, H2O2, NO• and •OH radicals indirectly. This element replaces Fe and Cu from proteins (ferritin), which releases free Fe2+ and Cu2+ ions, which cause oxidative stress. Acute Cd intoxication has revealed increased activity of antioxidant defense enzymes such as catalase, Cu-Zn superoxide dismutase, glutathione reductase, glutathione peroxidase and glutathione-S-transferase [48].
Combination therapy by using chelating agents with antioxidant supplementations like N-acetylcysteine, lipoic acid, melatonin, gossypin etc., have shown considerable beneficial promise providing improved clinical recovery. Along with antioxidant activity, N-acetylcysteine is recognized to have chelating properties and has been applied in combined administrations with succimer, MiADMSA/DMSA in as and Pb intoxications. The combination of vitamin C with MiADMSA successfully detoxifies arsenic. Lipoic acid also interferes with the Pb and as absorption. Many studies have been described in which the co-administration of dietary nutrients like vitamins (thiamine), essential metals viz. Zn, Fe, phenolic compounds (quercetin) and amino acids (methionine) with chelating agents leads to various beneficial effects [49]. Vitamins C and E, essential biogenic metals, amino acid supplementations during chelation therapy have been found to be valuable and effective in growing metal mobilization and providing recovery [50-53].
Radioprotection
Biotransformation, associated with the action of strong oxidants, are destructive to proteins which changes the oxidation state of sulfur to maximum value of +6. Oxidizing agents, such as hydrogen peroxide, oxidize disulfide bridges and sulfhydryl groups of proteins into sulfo-groups R-SO3H, which means their denaturation. With radiation damage to cells, their redox potential can be changed. The stable aminothiol, beta-mercapto ethylamine (Mercaptamine) with a formula NH4CH2CH2SH, is used to maintain the potential as a radioprotector that defends the body from radiation damage. The sulfide group can participate in homolytic processes with the formation of low-reactive radicals R-S. This property of mercaptamine also serves as a protection against the action of free radical particles - products of radiolysis of water. Consequently, the equilibrium of thiol-disulfide is associated with the regulation of the activity of enzymes and hormones, the adaptation of tissues to the action of oxidants, reducing agents and radical particles.
Conclusion
Toxic heavy metals interact with the function of vital cations, cause enzyme inhibition, and generate oxidative stress. Depending on the lipophilicity of a metal-chelator complex, chelating agents may change the metal’s distribution in the body, and thereby potentially modify its toxicity. Chelation of free metal ions with polydentate ligands turns them into stable, more coordinated saturated particles that are not able to destroy biocomplexes, and therefore low-toxic. They are membrane permeable, capable of transportation and excretion from the body. So, the toxicity of an element is determined by its nature, dose and molecular form in the composition of which the element is located.
The recommended antidots for lead intoxication are CaNa2EDTA, CaNa2EDTA with BAL and DMSA in most of cases. Dimercaprol, penicillamine succimer or DMSA are successful antidots in cases of human arsenic intoxication. CaNa2EDTA is also recommended but with no proven clinical benefits. CaNa3DTPA, an efficient cobalt antidote, is also found active against acute Cd toxicity. Various carbodithioate derivatives including diethyl, dimethyl, diisopropyl-dithiocarbamates have been studied for their chelation efficacy against Cd toxicity. Combinations of DMSA with MiADMSA, DMSA with CaDTPA, N-acetyl cysteine with DMPS have been effectively used in acute Cd toxicity. Dimercaprol and D-penicillamine are usually prescribed chelators against elemental and inorganic Hg intoxication. Hydrophilic derivatives of DMPS, BAL and DMSA have been successfully established for the treatment of toxicity by organomercury compounds. It has to be noted that BAL may be contraindicated in poisoning by organomercury (phenyl-Hg and alkyl-Hg) compounds because the produced lipid soluble complex increases Hg circulation. The important role of heavy metals in oxidative damage proposed new strategies for treatment with proven antioxidants in modifying metal toxicity, and providing complicomplimentary chelating properties thus increasing the efficacy of the common chelators.
Acknowledgments: The author thanks the Bulgarian National Science Fund (Contract No. BG-RRP-2.004-0004-C01 of the Bulgarian National Recovery and Resilience Plan).
References
- Kim JJ, Kim YS, Kumar V. Heavy metal toxicity: An update of chelating therapeutic strategies. Journal of Trace elements in Medicine and Biology. 2019; 54: 226-231.
- Ponka P, Tenenbein M, Eaton JW. Iron. In Handbook on the Toxicology of Metals, 3rd ed, Nordberg GF, Fowler BA, Nordberg M, Friberg L, Eds, Academic Press: San Diego, CA, USA. 2007; 577-598.
- Kostova I, Soni RK. Bioinorganic Chemistry. Shree Publishers & Distributors: New Delhi, India. 2011.
- Goswami AK, Kostova I. Medicinal and Biological Inorganic Chemistry. Walter de Gruyter Gmb H & Co KG, 2022.
- Matović V, Buha A, Dukić-Ćosić D, Bulat Z. Insight into the oxidative stress induced by lead and/or cadmium in blood, liver and kidneys. Food and Chemical Toxicology. 2015; 78: 130–140.
- Bjørklund G, Crisponi G, Nurchi VM, Cappai R, Buha Djordjevic A, et al. A review on coordination properties of thiol-containing chelating agents towards mercury, cadmium, and lead. Molecules. 2019; 24: 3247.
- Andjelkovic M, Djordjevic AB, Antonijevic E, Antonijevic B, Stanic M, et al. Toxic effect of acute cadmium and lead exposure in rat blood, liver, and kidney. International Journal of Environmental Research and Public Health. 2019; 16: 274.
- Nurchi VM, Buha Djordjevic A, Crisponi G, Alexander J, Bjørklund G, et al. Arsenic toxicity: molecular targets and therapeutic agents. Biomolecules. 2020; 10: 235.
- Flora SJS. Preventive and therapeutic strategies for acute and chronic human arsenic exposure. Arsenic in drinking water and food. 2020; 341-370.
- Rajavardhan R, Mamadapur A, Shyamala N. A Rare Case. International Journal of Medical and Dental Sciences. 2021; 1961–1965.
- Prakash S, Verma AK. Arsenic: It’s Toxicity and Impact on Human health. International Journal of Biological Innovations. 2021; 3: 38-47.
- Zhang H, Reynolds M. Cadmium exposure in living organisms: A short review. Science of the Total Environment. 2019; 678: 761–767.
- Mezynska M, Brzóska MM. Environmental exposure to cadmium—a risk for health of the general population in industrialized countries and preventive strategies. Environmental Science and Pollution Research. 2018; 25: 3211–3232.
- Remelli M, Nurchi VM, Lachowicz JI, Medici S, Zoroddu MA, et al. Competition between Cd (II) and other divalent transition metal ions during complex formation with amino acids, peptides, and chelating agents. Coordination Chemistry Reviews. 2016; 327–328: 55–69.
- Satarug S, Vesey DA, Gobe GC. Current health risk assessment practice for dietary cadmium: Data from different countries. Food and Chemical Toxicology. 2017; 106: 430–445.
- Djordjevic VR, Wallace DR, Schweitzer A, Boricic N, Knezevic D, et al. Environmental cadmium exposure and pancreatic cancer: Evidence from case control, animal and in vitro studies. Environment International. 2019; 128: 353–361.
- Rahimzadeh MR, Rahimzadeh MR, Kazemi S, Moghadamnia AA. Cadmium toxicity and treatment: An update. Caspian Journal of Internal Medicine. 2017; 8: 135.
- Bjørklund G, Lindh U, Aaseth J, Mutter J, Chirumbolo S. Mercury in dental amalgams: A great concern for clinical toxicology in developing countries? Journal of Trace elements in Medicine and Biology. 2019; 51: 9–11.
- Bjørklund G, Tinkov AA, Dadar M, Rahman MM, Chirumbolo S, et al. Insights into the Potential Role of Mercury in Alzheimer’s Disease. Journal of Molecular Neuroscience. 2019; 67: 511–533.
- Cariccio VL, Samà A, Bramanti P, Mazzon E. Mercury involvement in neuronal damage and in neurodegenerative diseases. Biological Trace Element Research. 2019; 187: 341–356.
- Amadi CN, Offor SJ, Frazzoli C, Orisakwe OE. Natural antidotes and management of metal toxicity. Environmental Science and Pollution Research. 2019; 26: 18032-18052.
- Bjørklund G, Dadar M, Mutter J, Aaseth J. The toxicology of mercury: Current research and emerging trends. Environmental Research. 2017; 159: 545–554.
- Aaseth J, Crisponi G, Anderson O. Chelation Therapy in the Treatment of Metal Intoxication; Academic Press: Cambridge, MA, USA, 2016.
- Nurchi VM, Crespo-Alonso M, Toso L, Lachowicz JI, Crisponi G. Chelation Therapy for Metal Intoxication: Comments from a Thermodynamic Viewpoint. Mini-Reviews in Medicinal Chemistry. 2013; 13: 1541–1549.
- Bjørklund G, Mutter J, Aaseth J. Metal chelators and neurotoxicity: Lead, mercury, and arsenic. Archives of Toxicology. 2017; 91: 3787–3797.
- Bradberry S, Vale A. Dimercaptosuccinic acid (succimer; DMSA) in inorganic lead poisoning. Clinical Toxicology. 2009; 47: 617–631.
- De La Gala Morales M, Ariño C, Díaz-Cruz JM, Esteban M. Study of the complexation of Pb (II) with meso-2,3-Dimercaptosuccinic Acid (DMSA) and 2,3-dimercapto-1-propanesulfonic acid (DMPS) using a bismuth-bulk rotating disk electrode. Electroanalysis. 2014; 26: 1912–1919.
- Gersl V, Hrdina R, Vavrova J, Holeckova M, Palicka V, et al. Effects of repeated administration of dithiol chelating agent- sodium 2,3-dimercapto 1-propanesulphonate (DMPS)- on biochemical and hematological parameters in rabbits. Acta Medica. 1997; 40: 3-8.
- Walker EM, Stone A, Milligan LB, Gale GR, Atkins LM, et al. Mobilization of lead in mice by administration of monoalkyl esters of meso-2, 3-dimercaptosuccinic acid. Toxicology. 1992; 76: 79-87.
- Flora SJS, Bhadauria S, Pachauri V, Yadav A. Monoisoamyl 2, 3-Dimercaptosuccinic Acid (MiADMSA) Demonstrates Higher Efficacy by Oral Route in Reversing Arsenic Toxicity: A Pharmacokinetic Approach. Basic & Clinical Pharmacology & Toxicology. 2012; 110: 449–459.
- Taubeneck MW, Domingo JL, Llobet JM, Keen CL. Meso 2, 3-Dimercaptosuccinic Acid (DMSA) affects maternal and fetal copper metabolism in Swiss mice. Toxicology. 1992; 72: 27-40.
- Flora SJS, Pande M, Kannan GM, Mehta A. Lead induced oxidative stress and its recovery following co-administration of melatonin or N-acetylcysteine during chelation with succimer in male rats. Cellular and Molecular Biology. 2004; 50: 543-551.
- Bjørklund G, Aaseth J, Crisponi G, Rahman MM, Chirumbolo S. Insights on alpha lipoic and dihydrolipoic acids as promising scavengers of oxidative stress and possible chelators in mercury toxicology. Journal of Inorganic Biochemistry. 2019; 195: 111–119.
- Horn N, Møller LB, Nurchi VM, Aaseth J. Chelating principles in Menkes and Wilson diseases: Choosing the right compounds in the right combinations at the right time. Journal of Inorganic Biochemistry. 2019; 190: 98–112.
- Roussaeux CG, MacNabb LG. Oral administration of D-pencillamine causes neonatal mortality without morphological defects in CD-1 mice. Journal of Applied Toxicology. 1992; 12: 35-38.
- Walker EMJr, Gale GR, Fody EP, Atkins LM, Smith AB, et al. Comparative antidotal effects of diethyldithicarbamate, dimercaptosuccinate and diethylene triamine pentaacetate against cadmium induced testicular toxicity in mice. Research communications in chemical pathology and pharmacology. 1986; 51: 231-244.
- Winship KA. Toxicity of aluminium: A historical review. Adverse Drug Reactions and Toxicological Reviews. 1993; 12: 177-211.
- Hoffbrand AV, Cohen A, Hershko C. Role of deferiprone in chelation therapy for transfusional iron overload. Blood. 2003; 102: 17-24.
- Kattamis A, Ladis V, Berdousi H, Kelekis NL, Alexopoulou E, et al. Iron chelation treatment with combination therapy with deferiprone and deferioxamine: A 12-month trial. Blood Cells, Molecules, and Diseases. 2006; 36: 21-25.
- Andersen O. Principles and recent developments in chelation treatment of metal intoxication. Chemical Reviews. 1999; 99: 2683-2710.
- Kodama H, Murata Y, Iitsuka T, Abe T. Metabolism of administered triethylene tetramine dihydrochloride in humans. Life Sciences. 1997; 61: 899-907.
- Bahnemann R, Leibold E, Kittel B, Mellert W, Jackh R, et al. Different patterns of kidney toxicity after sub-acute administration of Na-nitrilotriacetic acid and Fe-nitrilotriacetic acid to Wistar rats. Toxicological Sciences. 1998; 46: 166-175.
- Kargačin B, Kostial K, Arežina R, Singh PK, Jones MM, Cikrt M. Influence of age and time of administration of dithiocarbamate analogues on cadmium retention in rats. Journal of Applied Toxicology. 1991; 11: 273–277.
- Mishra D, Mehta A, Flora SJS. Reversal of hepatic apoptosis with combined administration of DMSA and its analogues in guinea pigs: role of glutathione and linked enzymes. Chemical Research in Toxicology. 2008; 21: 400-407.
- Bhadauria S, Flora SJS. Response of arsenic induced oxidative stress, DNA damage and metal imbalance to combined administration of DMSA and monoisoamyl DMSA during chronic arsenic poisoning in rats. Cell Biology and Toxicology. 2007; 23: 91-104.
- Aaseth J, Ajsuvakova OP, Skalny AV, Skalnaya MG, Tinkov AA, et al. Chelator combination as therapeutic strategy in mercury and lead poisonings. Coordination Chemistry Reviews. 2018; 358: 1–12.
- Pi J, Horiguchi S, Sun Y, Nikaido M, Shimojo N, Hayashi T. A potential mechanism for the impairment of nitric oxide formation caused by prolonged oral exposure to arsenate in rabbits. Free Radical Biology and Medicine. 2003; 35: 102-113.
- Ognjanovic BI, Pavlovic SZ, Maletic SD, Zikic RV, Stajn AS, et al. Protective influence of vitamin E on antioxidant defense system in the blood of rats treated with cadmium. Physiological Research. 2003; 52: 563-570.
- Flora SJS, Pachauri V. Chelation in Metal Intoxication. International Journal of Environmental Research and Public Health. 2010; 7: 2745-2788.
- Pachauri P, Saxena G, Mehta A, Mishra D, Flora SJS. Combinational chelation therapy abrogates lead induced neurodegeneration in rats. Toxicology and Applied Pharmacology. 2009; 240: 255-265.
- Flora SJS, Pande M, Mehta A. Beneficial effect of combined administration of some naturally occurring antioxidants (vitamins) and thiol chelators in the treatment of chronic lead intoxication. Chemico-Biological Interactions. 2003; 145: 267-280.
- Pande M, Flora SJS. Lead induced oxidative damage and its response to combined administration of α-lipoic acid and succimers in rats. Toxicology. 2002; 177: 187-196.
- Flora SJS, Mittal M, Mehta A. Heavy metal induced oxidative stress & it’s possible reversal by chelation therapy. Indian Journal of Medical Research. 2008; 128: 501-523.