
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Retained large intraorbital metallic foreign body with delayed presentation: An unusual case report
Md Shahid Hasan Khan*; Fateha Yasmin Antara; Avijit Dey; Sheikh Mahmood Hasan; Md Mahmudul Haque Morshed; Md Nuruzzaman Khan; Saumitra Sarkar
Department of Neurosurgery, Shaheed Suhrawardy Medical College Hospital, Dhaka, Bangladesh.
*Corresponding Author : Md Shahid Hasan Khan
Indoor Medical Officer, Department of Neurosurgery, Shaheed Suhrawardy, Medical College Hospital, Dhaka, Bangladesh.
Tel: +88-01812030134;
Email: nishat.doc@gmail.com
Received : Dec 15, 2022
Accepted : Jan 06, 2023
Published : Jan 13, 2023
Archived : www.jcimcr.org
Copyright : © Hasan Khan S (2023).
Abstract
Penetrating orbital trauma necessitates a multidisciplinary approach because complex orbital injuries often encompass damage to the brain, the eyes, and the disfigurement of the face. The prognosis depends on the location of the injury, the type and size of the foreign body, and the subsequent complications. Given that this kind of trauma is a surgical emergency, a thorough evaluation involving a comprehensive history, meticulous examination to determine the mechanism and origin of the trauma, appropriate imaging studies to identify the exact location of the FB, and a timely referral to a specialty hospital are essential for prompt diagnosis and management to avoid complications related to delayed presentation. Here, we describe an unusual case of a large metallic foreign body that lodged inside the orbit following an incident of trauma while the patient was reasonably asymptomatic for four months. It is unusual since the foreign body is too large enough to cause symptoms, and a portion of it is clearly visible from the outside, but the patient’s presentation was delayed.
Keywords: Retained foreign body; Penetrating orbital injury; Orbital trauma; Intraorbital foreign body.
Citation: Hasan Khan S, Antara FY, Dey A, Hasan SM, Morshed MMH, et al. Retained large intraorbital metallic foreign body with delayed presentation: An unusual case report. J Clin Images Med Case Rep. 2023; 4(1): 2241.
Introduction
Ocular trauma is a significant cause of blindness all over the world. Approximately 16% of cases of orbital trauma are associated with a foreign body [1]. The term “intraorbital foreign body” (IOFB) describes a foreign body that is within the bony orbital walls, posterior to the orbital septum, but outside the eyeball [2]. It frequently affects teenagers and is typically brought on by high-velocity craniofacial trauma forces such as work-related injuries, gunshot wounds, or even more minor injuries like regular domestic duties [3]. Even though some cases seem trivial, special attention must be paid to retained foreign bodies because underestimating trauma can have dangerous or potentially life-threatening effects, such as vision loss due to lesions of the eyeball, optic nerve, or their vasculature, lesions of the abducens or oculomotor nerves, orbital inflammation, orbital fistula, orbital compartment syndrome, or even pneumocephalus or meningitis [4]. Every case of orbital trauma should be checked for the presence of an intraorbital foreign body, and this diagnosis should be confirmed or ruled out on imaging because clinical signs at the anterior surface of the orbit can be sparse, nonspecific, like in orbital cellulitis, or delayed presentation after the orbital trauma when the entry wound is healed [4]. In this report, we describe a case of a retained intraorbital large metallic foreign body, where part of the object was visible from outside, that remained reasonably asymptomatic for the initial four months following a traumatic event. After a thorough evaluation, the patient later underwent surgical toileting, removal of the foreign body, and exenteration due to complete loss of vision and a painful eye. We think the presentation is unusual because, to the best of our knowledge, we haven’t found any other case with a similar presentation in our web search.
Case report
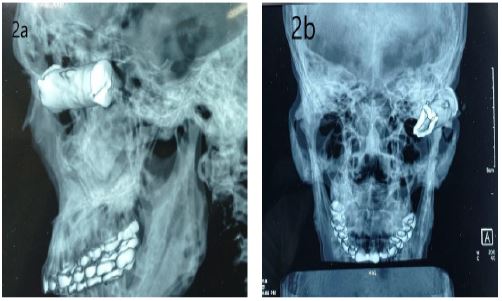
A 29-year-old male, a rickshaw puller by profession, hailing from a remote northern part of Bangladesh and belonging to a low socioeconomic status, presented with a 1-month history of left eye tearing, pain, occasional seropurulent discharge, and progressive loss of vision. There was a history of a penetrating left orbital injury following a road traffic accident 5 months ago, which was treated by a local quack doctor. According to the statement of the patient, the wound was sutured, leaving a part of the foreign body, and he was advised to get admitted into a tertiary level hospital as a part of the foreign body could not be removed. The patient did not visit the hospital, as he had been reasonably asymptomatic for the initial 4 months following the incident of trauma, except for difficulty in left eye vision. On inspection, a part of the metal object was externally visible, penetrating the upper eyelid into the orbit with a healed wound scar surrounding the object (Figure 1). Ocular examination revealed complete loss of vision in the left eye. Slit lamp and fund us examination of the left eye reveal massive retinal detachment. An ophthalmological examination of the right eye reveals normal findings. Routine investigations were within normal limits, except for raised WBC and ESR. An orbital X-ray revealed a large radiopaque shadow in the left orbit (Figures 2a,2b). For better delineation, a CT scan of the brain and orbit was done, which showed a large radiopaque metallic foreign body at the lateral aspect of the left orbital cavity and left eyeball, which could not be well evaluated due to metallic artifacts. However, it appears to be deformed (Figure 3a). CT-3D reconstruction shows large metallic foreign body at lateral aspect of the left orbital cavity, y extending into the posterior segment of the eye causing a comminuted fracture at frontal bone forming roof of the orbit, zygomatic bone and post- traumatic encephalomalacic change at the left anterior frontal region, and a comminuted fracture at frontal bone forming roof of the orbit, zygomatic bone (Figure 3c). A multidisciplinary (MDT) meeting including neurosurgery, ophthalmology, and maxillofacial surgery departments was arranged, and a decision was made to go ahead with surgery. The patient underwent surgical toileting, removal of the metallic foreign body (41.5 cm) (Figure 5), fractured bony fragments, and exenteration through lateral orbitotomy. Orbital exenteration was done because of globe puncture, painful eye, and complete loss of vision. The patient’s overall general condition was normal postoperatively, and he made a quick recovery.


b. CT-3D reconstruction shows large metalic foreign body at lateral aspect of the left orbital cavity and comminuted fracture at frontal bone forming roof of the orbit and zygomatic bone.
c. Post traumatic encephalomalacic change at left anterior frontal bone forming roof of the orbit zygomatic.




Discussion
Foreign objects in orbit have the potential to become lodged in the orbital walls, which could cause harm to neighboring structures like the globe, cranial nerves (especially cranial nerves II, III, IV, V, and VI), and extraocular muscles. Even though it’s uncommon, an orbital foreign body can enter the orbit right through the globe and settle into the apex [5]. In our case, a large metallic foreign body measuring around 4 × 1.5 cm penetrated through the lateral aspect of the upper eyelid into the posterior aspect of the left orbital cavity and injured the globe with a comminuted fracture at the frontal bone forming the roof of the orbit and zygomatic bone following an incident of RTA. There are very few articles on this topic, especially when it is located posteriorly in the orbit. In the study by Finkelstein et al., which was done retrospectively over a period of 7 years, they gathered a total of 27 patients with such injuries, all involving only metallic foreign bodies. Results of this study showed that 13 projectiles were lodged anteriorly, 4 were in an epibulbar position, and the remaining 10 were posterior to the equator. Out of these, all except one of anterior and 8 of posterior positions were operated. It shows that 80 percent of posterior positioned foreign bodies were not operated and safely left behind 6. Another review of 40 patients seen at two regional orbital surgery departments with intraorbital foreign bodies was done by Fulcher et al. Out of them, 22 had metallic -inorganic; 5 had nonmetallic - inorganic; and 13 had organic intraorbital foreign bodies. All of them had surgery except for 6 patients as they had posteriorly located inorganic foreign bodies. They concluded that posteriorly located inorganic IOFB should be treated conservatively unless it causes major orbital complications [7]. In another case highlighted that Inorganic foreign bodies on the other hand should be removed if located anteriorly and freely palpable. Non-palpable anterior, epibulbar and posterior foreign bodies can be managed conservatively given the risk of further damage during surgical extraction [8]. In our case, the patient was initially treated by a local quack doctor. The foreign body was partially left behind in the wound after it was sutured. He was advised to visit a higher level hospital because the foreign body could not be completely removed. Despite having a large metallic foreign body that is visible from outside, he didn’t seek medical help further as he had been reasonably asymptomatic for the initial 4 months following the incident of trauma except for difficulty in left eye vision, which he overlooked. This is not so unusual in a third-world country like Bangladesh, where many remote parts of the country are too impoverished to get even primary healthcare services. On top of that, patients’ negligence and a delayed referral system are equally responsible for the delayed presentation. A patient with an orbital foreign body may occasionally experience no symptoms since it is an occult foreign body. Patients may present with double vision, discomfort, edema, or visual abnormalities [5]. Our patient remained reasonably asymptomatic for the first 4 months, and then he gradually developed eye tearing, pain, occasional seropurulent discharge, and progressive loss of vision and presented to our neurosurgery department. With no delays, a decision for surgery was made after liaising with the ophthalmology and maxillofacial surgery departments. Regarding management, the principles of advanced trauma support must be followed in any trauma case. Removal of the foreign body should be postponed until a physical examination and a full radiological evaluation are completed. Early removal of the foreign body outside of the controlled situation and the operating room may lead to a fatal hemorrhage [9,10]. In our case, the principles had not been followed; rather, an endeavor was made to remove the FB, which could have led to a fatal situation. If the patient could have been referred to us, an appropriate immediate intervention could have saved the patient’s vision. Facial and orbital trauma can precipitate vision-threatening injuries. In the case of the ruptured globe, primary surgical exploration and repair should be attempted; however, with an unsalvageable eye, there is no consensus in the literature as to whether orbital exenteration is the best treatment [11]. But during the presentation to us it was already too late to do immediate surgical exploration, removal of the FB, and repair of the globe to minimize loss of vision. In our case, the patient underwent surgical toileting, the removal of the metallic foreign body, broken bony fragments, and a modified orbital exenteration done through a lateral orbitotomy because of the painful eye, complete blindness, and intraoperative evidence of globe perforation. Modified orbital exenteration is a surgical technique that consists of the removal of the entire intraocular contents while preserving the eyelids [12].
Conclusion
Not all penetrating intraorbital foreign bodies appear right away after the occurrence. Every incidence of orbital trauma should be promptly investigated for the possibility of an intraorbital FB. Through evaluation involving proper history-taking, physical examination, appropriate imaging modality, and most importantly, an early referral to the specialty center and timely intervention, it is necessary to minimize the chances of complications.
Declarations
Conflicts of interest: There were no conflicts of interest, according to the authors, during the planning and writing of this paper.
Financial support and sponsorship: The authors of this study declare no sources of funding for this study.
Consent: Consent was obtained from the patient to write and publish this article and to use his photo.
References
- Khanam S, Agarwal A, Goel R, Rathie N, Raut A, et al. Clinical presentation and management strategies in intraorbital foreign bodies. Case Reports in Ophthalmological Medicine. 2021; 2021.
- Okonkwo SN, Agweye CT, Echieh CI. Penetrating orbital injury with retained metallic foreign body. Nigerian Journal of Medicine. 2022; 31: 359-361.
- Mirzaei F, Salehpour F, Shokuhi G, Asvadi Kermani T, Salehi S, et al. An unusual case of intra orbital foreign body; diagnosis, management, and outcome: a case report. BMC surgery. 2019; 19: 1-6.
- Szabo B, Pascalau R, Bartoè D, Bartos A, Szabo I, et al. Intraorbital penetrating and retained foreign bodies neurosurgical case series. Turk Neurosurg. 2019; 29: 538-548.
- Schmuter G, Stern EM, Packles M. Considerations for a Retained Foreign Body in the Posterior Orbital Apex. Cureus. 2021; 13.
- Finkelstein M, Legmann A, Rubin PA et al. Projectile metallic foreign bodies in the orbit: A retrospective study of epidemiologic factors, management, and outcomes; Ophthalmology. 1997; 104: 96-103.
- Fulcher TP, McNab AA, Sullivan TJ. Clinical features and management of intraorbital foreign bodies; Ophthalmology. 2002; 109: 494-500.
- Robert JP, Christopher Z, Gary JL. Jr. Posterior Intraorbital Foreign Body: Take it or Leave it? Open Reconstructive and Cosmetic Surgery. 2008; 1: 1-31.
- Turbin RE, Maxwell DN, Langer PD, Frohman LP, Hubbi B, et al. Patterns of transorbital intracranial injury: A review and comparison of occult and non-occult cases. Survey of ophthalmology. 2006; 51: 449–460.
- Swanson JL, Augustine JA. Penetrating intracranial trauma from a fishhook. Annals of emergency medicine. 1992; 21: 568–571.
- Barouj MD, Tabrizi R, Behnia P, Tabrizi MA, Kheirkhahi M, et al. Penetrating Orbital Injury; a Case Report and Treatment. Algorithm. Archives of academic emergency medicine. 2020; 8.
- Dey AK, Ray A, Banerjee R, Kole L, Paul S, et al. Management of Midface Fracture with Orbital Exenteration- A Case Report. IOSR Journal of Dental and Medical Sciences. 2022; 21: 09-15.