
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Giant abdominal cerebrospinal fluid pseudocystis: A rare complication of ventriculoperitoneal shunt
Maria Elena Pugliese*; Riccardo Battaglia; Girolama Raso; Orazio Francesco Antonio Carallo
Severe Acquired Brain Injury Unit, S.Anna Institute, 88900 Crotone, Italy.
*Corresponding Author : Maria Elena Pugliese
Severe Acquired Brain Injury Unit, S.Anna Institute, 88900 Crotone, Italy.
Email: me.pugliese@isakr.it.
Received : Dec 14, 2022
Accepted : Jan 09, 2023
Published : Jan 16, 2023
Archived : www.jcimcr.org
Copyright : © Pugliese ME (2023).
Citation:Pugliese ME, Battaglia R, Raso G, Carallo OFA. Giant abdominal cerebrospinal fluid pseudocystis: A rare complication of ventriculoperitoneal shunt. J Clin Images Med Case Rep. 2023; 4(1): 2243.
Description
Hydrocephalus is a condition that results from increased intracranial pressure. It can be caused by various conditions, including intracranial tumors, brain malformations, as well as disturbances in cerebrospinal fluid production and drainage. However, regardless of etiology, ventriculoperitoneal (VP) shunt is a common procedure used to reduce intracranial pressure. Abdominal cerebrospinal fluid pseudocyst, which is potentially life threatening, is a rare complication [1-4].
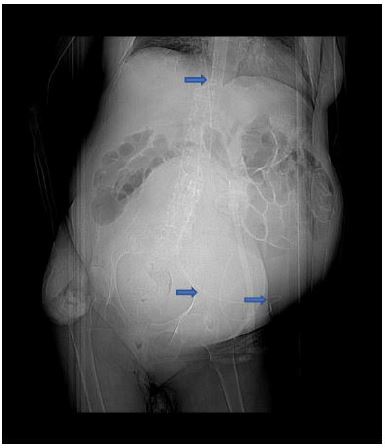
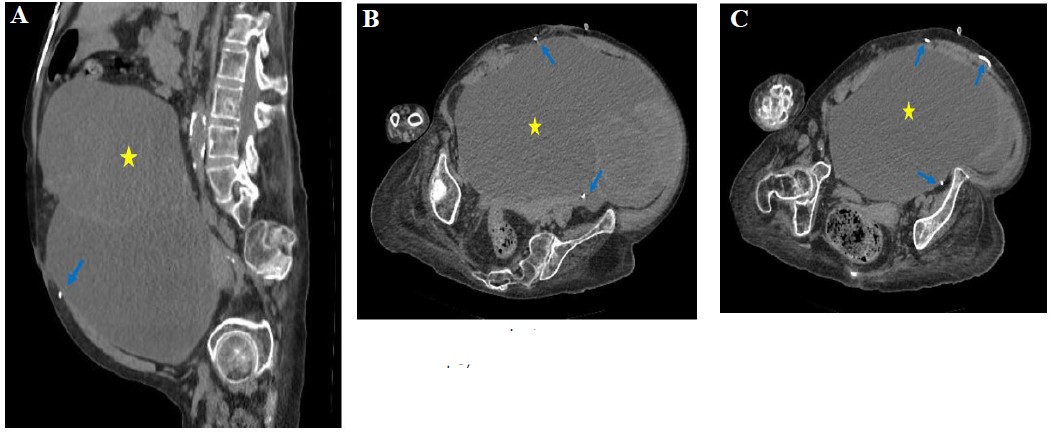
We describe the case of a 58 years old woman of our long-term care facility with abnormal abdominal distension and vomiting. The patient suffered of post-intracranial haemorragy vegetative state with consequent hydrocephalus treated with ventriculoperitoneal shunt placement seven years before. Physical examination revealed a large elastic palpable mass in the lower abdomen. No neurological change was observed. The patient underwent unenhanced abdominal computed tomography (CT). Abdominal CT revealed large homogeneous low-density fluid collection, 30 x 17 cm maximum diameter. The VPS catheter tip was adjacent to the fluid collection, suggesting a giant cystic lesion around the shunt catheter (Figure 1, figure 2 A, B, C). The cystic mass was independent of the pancreas and kidneys. Thus, a peritoneal pseudocyst around the VPS was suspected. The patient underwent surgical evaluation for ultra ultrasound-guided cystis aspiration because of poor prognosis that did not allow open surgical treatment.
In conclusion, this report describes an adult case of huge abdominal pseudocyst as a complication of ventriculoperitoneal shunt. Physicians awareness of this rare but possible complication is of crucial importance for early diagnosis and treatment.
References
- Sena FG, Sousa RM, Meguins LC. Abdominal cerebrospinal fluid pseudocyst: A complication of ventriculoperitoneal shunt in a Brazilian Amazon woman. Case report. Il Giorn Chir. 2010; 31: 371-373.
- Pernas JC, Catala J. Case 72: Pseudocyst around ventriculoperitoneal shunt. Radiology. 2004; 232: 239-243.
- Comba A, Gulenc N, Caltepe G, Dağçınar A, Yüce O, et al. Ascites and abdominal pseudocyst: Two uncommon ventriculoperitoneal shunt complications in two cases. Turk J Pediatr. 2013; 55: 655-658.
- Aparici-Robles F, Molina-Fabrega R, Abdominal cerebrospinal fluid pseudocyst: A complication of ventriculoperitoneal shunts in adults. J Med Imaging Radiat Oncol. 2008; 52: 40-43.