
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Lhermitte-Duclos disease: A case report
Wenjie Wang*; Zhifeng Wang
Department of Neurosurgery, Second Affiliated Hospital of Nantong University, North Haierxiang Road 6, Nantong 226001, Jiangsu Province, China.
*Corresponding Author : Wenjie Wang
Department of Neurosurgery, Second Affiliated Hospital of Nantong University, North Haierxiang Road 6, Nantong 226001, Jiangsu Province, China.
Email: 1394910671@qq.com
Received : Dec 22, 2022
Accepted : Jan 11, 2023
Published : Jan 18, 2023
Archived : www.jcimcr.org
Copyright : © Wang W (2023).
Citation: Marinova L, Georgiev R, Evgeniev N. Clinical observations in three clinical cases with locally advanced chordomas. What is needed for early diagnosis with improved survival?. J Clin Images Med Case Rep. 2020; 1(1): 1005.
Description
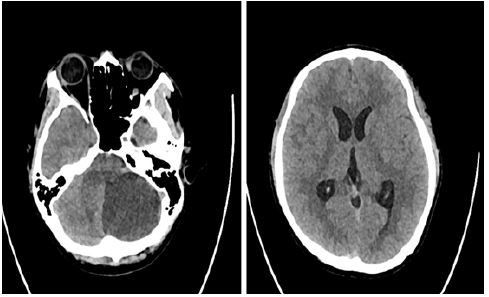
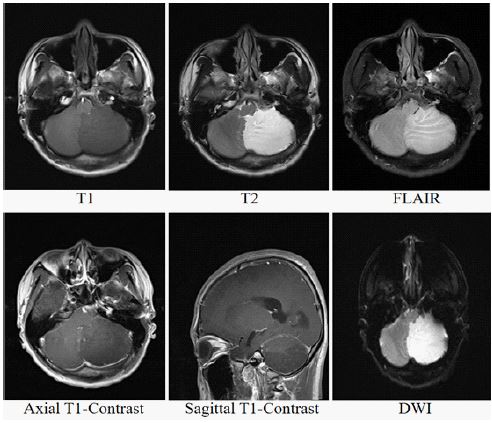
A 25-year-old young man came to the emergency department of our hospital with sudden dizziness and vomiting for one day. The neurologist performed a physical examination of the patient, found no positive signs, and ordered the patient to perform a head Computed Tomography (CT) examination, which showed a left cerebellar hemisphere mass with obstructive hydrocephalus (Figure 1). After admission, the brain Magnetic Resonance Imaging (MRI) was performed, and the results showed that the left cerebellar hemisphere showed low signal in T1, hyperintense signal in T2, FLAIR and DWI, and no significant enhancement of cerebellar lesion on T1-contrast scan (Figure 2). The pathological results of postoperative cerebellar specimens showed focal hyperplasia of neuronal cells in the cerebellar granule cell layer, Syn (synapsin) (+), NF (neurofilament) (+), GFAP (glial fibrillary acidic protein) (-), Ki67 (< 1%). Pathology considered dysplastic cerebellar gangliocytoma.
Discussion
Lhermitte-Duclos Disease (LDD), also called dysplastic cerebellar gangliocytoma, is a slow-progressing, rare benign cerebellar mass with features of hamartomas and true tumors, belonging to neuronal and mixed neuron-glial tumors [1]. LDD is closely related to Cowden syndrome, an autosomal dominant disorder caused by the PTEN (Phosphatase and tensin homolog) gene germline [2]. The cerebellar granule cell layer contains densely stained granule cells and Golgi cells. In the path ological state, the granule cell layer and the Purkinje cell layer are replaced by large abnormal neurons, and the molecular layer is myelinated and widened, and abnormally parallel myelinated fibers appear [3]. Pathologically, neuronal related immunological indicators such as Syn, NSE (neuron-specific enolase) and NF are positive due to the presence of neuronal cells in the cerebellar granule cell layer. LDD has low proliferative activity, so Ki67 is negative [4]. LDD occurs more often in young people, and its symptoms progress slowly, mainly manifested as cerebellar dysLhermitte-Duclos Disease (LDD), also called dysplastic cerebellar gangliocytoma, is a slow-progressing, rare benign cerebellar mass with features of hamartomas and true tumors, belonging to neuronal and mixed neuron-glial tumors [1]. LDD is closely related to Cowden syndrome, an autosomal dominant disorder caused by the PTEN (Phosphatase and tensin homolog) gene germline [2]. The cerebellar granule cell layer contains densely stained granule cells and Golgi cells. In the path ological state, the granule cell layer and the Purkinje cell layer are replaced by large abnormal neurons, and the molecular layer is myelinated and widened, and abnormally parallel myelinated fibers appear [3]. Pathologically, neuronal related immunological indicators such as Syn, NSE (neuron-specific enolase) and NF are positive due to the presence of neuronal cells in the cerebellar granule cell layer. LDD has low proliferative activity, so Ki67 is negative [4]. LDD occurs more often in young people, and its symptoms progress slowly, mainly manifested as cerebellar dysfunction, such as dizziness, vomiting and unsteady walking [5]. A characteristic “tiger stripes” may appear on MRI, because the atrophy of cerebellar central white matter forms a loose gap that makes the cerebrospinal fluid signal appear streaked. Because of the poor blood supply, the lesion is not significantly enhanced on contrast scanning [6]. LDD is mainly treated surgically, and the prognosis is generally acceptable [7].
References
- Otheman Y, Aalouane R, Aarab C, Rammouz I. A case report of Lhermitte-Duclos disease revealed by psychiatric disturbances. Ann Gen Psychiatry. 2017; 16: 24.
- Stambolic V, Suzuki A, de la Pompa JL, Brothers GM, Mirtsos C, et al. Negative regulation of PKB/Akt - dependent cell survival by the tumor suppressor PTEN. Cell 1998; 95: 29.
- Moonis G, Ibrahim M, Melhem ER. Diffusion-weighted MRI in Lhermitte-Duclos disease: Report of two cases. Neuroradiology. 2004; 46: 351-354.
- Thomas B, Krishnamoorthy T, Radhakrishnan VV, Kesavadas C. Advanced MR imaging in Lhermitte-Duclos disease: Moving closer to pathology and pathophysiology. Neuroradiology. 2007; 49: 733-738.
- Oppenheimer DR. A benign ‘tumor’ of the cerebellum. Report on two cases of diffuse hypertrophy of the cerebellar cortex with a review of nine previously reported cases. J Neurol Neurosurg Psychiatry. 1955; 18: 199-213.
- Klisch J, Juengling F, Spreer J, Koch D, Thiel T, et al. Lhermitte-Duclos disease: Assessment with MR imaging, positron emission tomography, single-photon emission CT, and MR spectroscopy. AJNR Am J Neuroradiol. 2001; 22: 824-830.
- Masmoudi A, Chermi ZM, Marrekchi S. Cowden syndrome. J Dermatol Case Rep. 2011; 5: 8-13.