
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Carotid web: An under-diagnosed cause of recurrent ischemic strokes
Saima Bashir1,2*; Sebastian Remollo2; María Hernandez-Perez3; Meritxell Gomis3; Carlos Castaño2; Mikel Terceño1,2; Mariano Werner2
1Stroke Unit, Department of Neurology, Hospital Universitari Doctor Josep Trueta de Girona, Spain.
2Interventional Neuroradiology Unit, Department of Neurosciences, Hospital Germans Trias i Pujol, Badalona, Spain.
3Stroke Unit, Department of Neurosciences, Hospital Universitari Germans Trias i Pujol, Badalona, Spain.
*Corresponding Author : Saima Bashir
Stroke Unit, Department of Neurology, Hospital Universitari Doctor Josep Trueta de Girona, Spain.
Tel: +34-654141188;
Email: sbashir.girona.ics@gencat.cat
Received : Dec 22, 2022
Accepted : Jan 13, 2023
Published : Jan 20, 2023
Archived : www.jcimcr.org
Copyright : © Bashir (2023).
Abstract
Background: Carotid Webs (CW) are an under-diagnosed cause of embolic stroke especially in young patients with no vascular risk factors. Strokes associated with CW are frequently severe, with a high proportion of Large Vessel Occlusion (LVO). They are frequently considered cryptogenic, and sub sequently, treatment with aspirin is initiated as secondary prevention. However, strokes secondary to a CW have high recurrence rates despite antithrombotic therapy, where as carotid revascularization is effective in preventing recurrent strokes.ss
Methods: This is a single case report of a patient who presented to the emergency department with a right-hemispheric is chemic stroke due to LVO, requiring treatment with Mechanical Thrombectomy (MT). No specific cause was found and aspirin was initiated. Two months later, the patient presented to the emergency department with yet another right-hemispheric is chemic stroke due to LVO, which required treatment with MT. The presence of the CW was confirmed with the digital subtraction angiography performed during the treatment. A retrospective evaluation of the angio -CT performed during the first stroke showed the presence of the CW, which was initially over looked. The patient was then treated with carotid stenting and presented no further recurrences.
Conclusion: Physicians should systematically investigate the presence of a CW in patients with cryptogenic strokes. The high recurrence rate despite medical treatment highlights the importance of an early diagnosis in order to opt for a more aggressive treatment. Carotid revascularization seems safe and effective in preventing recurrences, and it should probably be recommended as a first-line treatment in these patients.
Keywords: Carotid web; Recurrent stroke; Secondary prevention; Cryptogenic stroke.
Abbreviations: CW: Carotid Web; NIHSS: National Institutes Of Health Stroke Scale; NCCT: Non-Contrast Computed Tomography; CTA: CT Angiography; MCA: Middle Cerebral Artery; ASPECTS: Alberta Stroke Program Early CT Score; MT: Mechanical Thrombectomy; TICI: Thrombolysis in Cerebral Infarction; MRI: Magnetic Resonance Imaging; ESUS: Embolic Stroke Of Undetermined Source; DSA: Digital Subtraction Angiography; CEA: Carotid End Arterectomy; CAS: Carotid Artery Stenting.
Citation: Bashir S, Remollo S, Perez MH, Gomis M, Castaño C, et al. Carotid web: An under-diagnosed cause of recurrent ischemic strokes. J Clin Images Med Case Rep. 2023; 4(1): 2251.
Case presentation
A patient with a previous history of smoking habit, dyslipidemia and migraine, presented to the emergency department with a right-hemispheric ischemic stroke. On arrival at that hospital, the National Institutes of Health Stroke Scale (NIHSS) was 15. The patient had a forced conjugate gaze deviation to the right, dysarthria, severe left hemiparesis and left hemianopia. She underwent a Non-Contrast Computed Tomographic (NCCT) examination of the brain along with a CT Angiography (CTA) of intracranial and extra cranial vessels. The NCCT showed early ischemic changes in the territory corresponding to the right Middle Cerebral Artery (MCA), with an Alberta Stroke Program Early CT Score (ASPECTS) of 8, and a chronic infarct in the corona radiata. The CTA demonstrated a proximal occlusion of the right MCA, with no signs of atherosclerotic disease in the extra cranial arteries. Treatment with Mechanical Thrombectomy (MT) was performed, achieving a successful recanalization (Thrombolysis In Cerebral Infarction (TICI) 2B), and the patient presented significant clinical improvement. An extensive etiological study was performed with blood tests, Magnetic Resonance Imaging (MRI) of the brain and angio-MRI, heart rate monitoring and echocardiography, but no specific cause was found. Treatment with aspirin and statins was therefore initiated, as the standard of care for any Embolic Stroke of Undetermined Source (ESUS). The patient was asymptomatic at discharge.
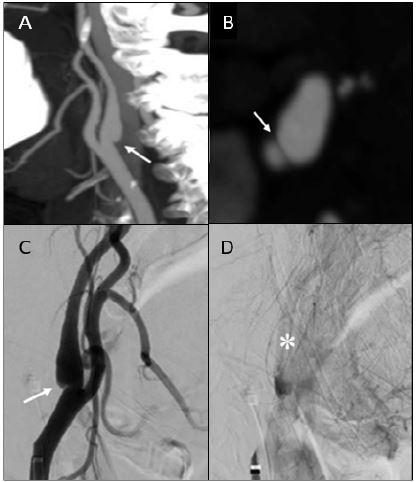
Two months later, the patient presented to the emergency department of our hospital with a right-hemispheric ischemic stroke, and an NIHSS of 14 on arrival. CT examination demonstrated a hyper acute ischemic lesion in the head of the right caudate nucleus (ASPECTS 9), and a chronic infarction in the MCA territory, corresponding to the previous stroke. CTA showed a proximal occlusion of the right MCA and a Carotid Web (CW) in the posterior wall of the internal carotid bulb (Figure 1). Treatment with MT was performed, and a final TICI score 2C was achieved. The presence of the CW was confirmed with the Digital Subtraction Angiography (DSA) performed during the MT. A retrospective evaluation of the CTA performed in the first hospital showed the presence of the CW, which was initially over looked.
The case was discussed in a multi disciplinary committee of our center, and treatment with carotid stenting was recommended. One week after stroke onset, the patient was treated with carotid stenting (Figure 1), with no complications during the procedure. The patient presented no further recurrences.
Discussion and conclusions
A Carotid Web (CW) is an atypical focal fibro muscular dysplasia, which was first described by Rainer et al [1]. In a case of recurrent left hemispheric events in an otherwise healthy young person. A CW appears as a shelf-like projection arising from the posterior wall of the proximal internal carotid artery bulb. Histological analysis reveals findings consistent with an intimal variant of fibro muscular dysplasia: Intimal fibrosis and hyperplasia, with the media being only minimally involved, presenting depletion of its elastic fibers replaced by fibrous tissue interspersed with muscle cells [1,2]. Additionally, histopathologic reports after surgical excision of CW show an absence of atherosclerotic disease [2,3].
CW has been recognized as an under diagnosed cause of cryptogenic stroke [1-3]. According to various studies, [2-7] patients with symptomatic CWs are mostly women, of African American origin, relatively young, and have a lower prevalence of vascular risk factors compared with those with other forms of is chemic stroke. Its incidence in the general population is unknown due to lack of specific studies. Prevalence of CW in patients with cryptogenic stroke varies across studies [2,4,6,7], ranging from 9.4% in patients < 60 years old to 37% in patients < 55 years old. A case-control study [4] reported an odds ratio estimate of 8.0 (95% CI: 1.2, 67) for the presence of symptomatic CW in stroke patients versus control subjects. Reported bilateral webs range from 8% [5] to 58% [7] of patients. It is likely that the mechanism of stroke is the recirculation of blood distal to the web causing blood stagnation in the diaphragm and an increase in platelet deposition and aggregation, which could lead to thrombogenesis, and, eventually, to distal embolization [2,8]. Thus, CW are often a cause of large is chemic strokes secondary to this artery-to-artery embolism. Due to this suggested mechanism, it is believed that the risk of stroke is independent of the degree of stenosis, which is rarely significant in CW [5,6].
Radio graphically CW appears on sagittal or oblique sagittal CTA as a thin filling defect arising from the posterior wall of the carotid bulb and projecting into the arterial lumen [2,3], and as a septum on axial CTA [5], with no signs of atherosclerosis, such as wall calcifications [2,3]. CW should be distinguished from the so called small protruding lesions [3], which are smaller, and do not present the axial septum. These small protruding lesions do not appear to present the same association with ischemic stroke as CW [5]. CTA is the diagnostic modality of choice [3] because it allows multiplane reconstruction, identification of possible thrombus at the web, and evaluation of atherosclerotic lesions. Additional information can be obtained on DSA, which permits the visualization of the flow stagnation just distal to the web in late phases. However, CW may not be visualized on DSA if only anterior–posterior or straight lateral projections are used, as is frequently the case in mechanical thrombectomy. Other diagnostic modalities such as MRI or ultrasound may be used for the identification of CW, but with lower sensitivity [9]. The lack of significant stenosis - and therefore, of hemodynamic effects on the carotid circulation-, the challenges in radiological identification of the web due to its size and origin, and the fact that it is more frequent in younger patients without cardiovascular risk factors, favors the under diagnosis of this entity. Radiographic differential diagnosis of CW must be done with arterial dissections, non-calcified atherosclerotic plaques and intraluminal thrombus [9]
According to several studies [2,3,6,7,10 ], CWs are associated with a high recurrence rate, ranging from 25% to 71.4%, despite medical therapy. Regarding treatment, to date the optimal management for an asymptomatic CW is unknown, and there are no recommendations on the best strategy for secondary prevention in a patient with a symptomatic CW. Medical treatment with antiplatelet therapy seems insufficient due to the high recurrence rate described [2,6,7]. Since the pathophysiologic mechanism of stroke suggested could be considered as analogous to the left atrial appendage in atrial fibrillation, in which there is a recirculation zone that causes stagnation of blood, anticoagulation seems more suitable than antiplatelet therapy. However, high rates of recurrent stroke have been described also in patients receiving anticoagulants [6]. A possible explanation for the relative inefficacy of medical therapy is that it has no remodeling effect on the web, and thus, the underlying substrate for recurrent stroke remains unchanged. It seems reasonable, therefore, to adopt a more aggressive strategy for secondary prevention. Both Carotid End Arterectomy (CEA) [2,6] and Carotid Artery Stenting (CAS) [6,7,10] have been reported to be safe and effective against stroke recurrence, with low procedural complication rates. In contrast with CAS, CEA has the advantage that pathological confirmation of the diagnosis of carotid web can be obtained after the procedure. In a systematic review of patients with CW and acute ischemic stroke [6], in which 160 patients with CW were included, the stroke recurrence rate was 54% in patients treated with antiplatelet therapy and 75% in anticoagulated patients, and the median time to recurrent stroke was 12 months. Seventy two per cent of patients with symptomatic CW were treated with carotid revascularization (CEA or CAS), either as a primary treatment for secondary stroke prevention or as a rescue treatment for patients experiencing a recurrent stroke despite medical management. No procedural complications were reported, and no patients presented a recurrent stroke during the median follow-up period of 14 months (range 3–144 months).
Conclusion
Awareness should be raised regarding CW, since it is an under-diagnosed cause of stroke. The high recurrence rates of stroke despite medical treatment with antiplatelet therapy or anti coagulation highlights the importance of a correct and early diagnosis in order to opt for a more aggressive treatment. Early carotid revascularization seems to be safe and effective in preventing recurrences, and it should probably be recommended as a first-line treatment in these patients. None the less, the data available regarding treatment derives mostly from observational studies; therefore, no formal recommendations can be done on the optimal management of symptomatic CW. Further research with randomized controlled studies regarding this issue is needed.
Declarations
Ethics approval and consent to participate: Need for approval by the ethics committee of our center was waived.
Consent for publication: The patient has provided written consent for publication.
Availability of data and materials: The datasets used during the current study are available from the corresponding author on reasonable request.
Competing interests: The authors declare that they have no competing interests.
Funding: No sources of funding.
Authors’ contributions: SB: Drafting/revision of the manuscript for content, including medical writing for content; Major role in the acquisition of data; Study concept or design; Analysis or interpretation of data.
SR: Drafting/revision of the manuscript for content, including medical writing for content.
MHP: Drafting/revision of the manuscript for content, including medical writing for content.
MG: Drafting/revision of the manuscript for content, including medical writing for content.
CC: Drafting/revision of the manuscript for content, including medical writing for content.
MT: Drafting/revision of the manuscript for content, including medical writing for content.
MW: Drafting/revision of the manuscript for content, including medical writing for content; Major role in the acquisition of data.
Acknowledgements: Not applicable
References
- Rainer WG, Cramer GG, Newby JP, Clarke JP. Fibro muscular hyperplasia of the carotid artery causing positional cerebral ischemia. Ann Surg. 1968; 167: 444-446.
- Joux J, Chausson N, Jeannin S. Carotid-bulb atypical fibro muscular dysplasia in young Afro-Caribbean patients with stroke. Stroke. 2014; 45: 3711-3713.Joux J, Chausson N, Jeannin S. Carotid-bulb atypical fibro muscular dysplasia in young Afro-Caribbean patients with stroke. Stroke. 2014; 45: 3711-3713.
- Choi PM, Singh D, Trivedi A. Carotid Webs and Recurrent Ischemic Strokes in the Era of CT Angiography. AJNR Am J Neuroradiol. 2015; 36: 2134-2139.
- Coutinho JM, Derkatch S, Potvin ARCarotid artery web and ischemic stroke: A case-control study [published correction appears in Neurology. 2017; 89: 521. Neurology. 2017; 88: 65-69.
- Compagne KCJ, van Es ACGM, Berkhemer OA. Prevalence of Carotid Web in Patients with Acute Intracranial Stroke Due to Intracranial Large Vessel Occlusion. Radiology. 2018; 286: 1000-1007.
- Zhang AJ, Dhruv P, Choi P. A Systematic Literature Review of Patients with Carotid Web and Acute Ischemic Stroke. Stroke. 2018; 49: 2872-2876.
- Haussen DC, Grossberg JA, Bouslama M, et al. Carotid Web (Intimal Fibromuscular Dysplasia) Has High Stroke Recurrence Risk and Is Amenable to Stenting. Stroke. 2017; 48: 3134-3137.
- Compagne KCJ, Dilba K, Postema EJ. Flow Patterns in Carotid Webs: A Patient-Based Computational Fluid Dynamics Study. AJNR Am J Neuroradiol. 2019; 40: 703-708.
- Mac Grory B, Emmer BJ, Roosendaal SD, Zagzag D, Yaghi S, et al. Carotid web: An occult mechanism of embolic stroke. J Neurol Neurosurg Psychiatry. 2020; 91: 1283-1289.
- Haussen DC, Grossberg JA, Koch S. Multicenter Experience with Stenting for Symptomatic Carotid Web. Interv Neurol. 2018; 7: 413-418.