
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Distal esophageal spasm (DES) can be achalasia in evolution: A case report
Tayyab Saeed Akhtar1 ; Ahsan Nawaz1; Gul Nisar1; Abdul Rauf Khan1; Sameen Abbas2*
1Center for Liver and Digestive Diseases, Holy Family Hospital Rawalpindi, Pakistan.
2Department of Pharmacy, Quaid-I-Azam University, Islamabad, Pakistan.
*Corresponding Author : Sameen Abbas
Department of Pharmacy, Quaid-I-Azam University, Islamabad, Pakistan.
Email: sameenabbas@bs.qau.edu.pk
Received : Dec 31, 2022
Accepted : Jan 16, 2023
Published : Jan 23, 2023
Archived : www.jcimcr.org
Copyright : © Abbas S (2023).
Abstract
Diffuse Esophageal Spasm (DES) and Achalasia have similar clinical and manometric traits. Though it might not happen often, certain reports seem to support the idea that DES can develop to achalasia. It is still difficult to determine the frequency of DES development to achalasia and the factors that influence this progression. An elderly man with dysphagia is the subject of a case study, and the manometry results showed a pattern shift from DES to Type II Achalasia. However, DES is still a difficult diagnosis to make from a clinical and manometric perspective.
Keywords: High-resolution manometry; Distal esophageal spasm; Achalasia; Case report.
Citation: Akhtar TS, Nawaz A, Nisar G, Khan AR, Abbas S, et al. Distal esophageal spasm (DES) can be achalasia in evolution: A Case Report. J Clin Images Med Case Rep. 2023; 4(1): 2252.
Introduction
With the introduction of High-Resolution Manometry (HRM) and the standardization of findings through the Chicago classification v.4.0, classification of esophageal motility disorders not only has become simpler but also makes it possible to gain more insight into the pathophysiology and connections between various motility disorders [1]. Distal Esophageal Spasm (DES) and Achalasia are two separate yet over-lapping entities like both having high amplitude simultaneous contractions of the esophagus. However, for DES the LES relaxation has to be normal, which is incomplete in subjects with Achalasia. This problem is made even more challenging by the possibility that DES will eventually proceed to achalasia, with the likelihood of aperistalsis following [2]. We present a case report of an elderly male presenting with dysphagia and his manometry findings revealed a shift of pattern from DES to Type II Achalasia.
Case report
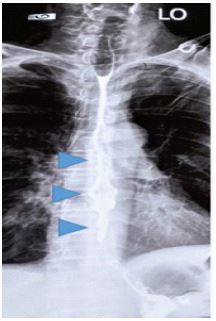
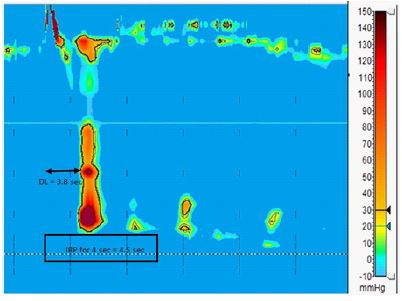
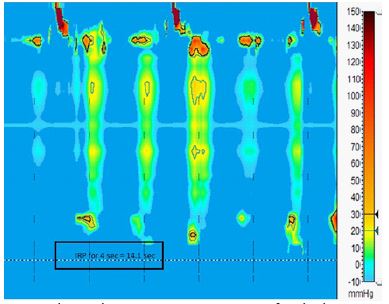
We discuss the case of an 80-year-old man who, for four years, experienced difficulty swallowing both solids and liquids. He underwent an upper GI endoscopy, and there was no sign of a mechanical obstruction. His Barium Swallow showed Corkscrew appearance of distal esophagus suggesting tertiary peristalsis movement (Figure 1). HRM was performed showing premature contractions with DL < 4.5 seconds and mean DL of 3.11 seconds (Figure 2). However, with the last two viscous swallows the pattern changed to pan-esophageal pressurizations (Figure 3). Overall, the mean IRP for 4 seconds was 9.354 mmHg (normal: 15 mmHg), but after DES, the mean IRP increased to 10.344 mmHg, and after pan-esophageal pressurization, it increased to 13.25 mmHg. The pan-esophageal pressurization that occurred during the final swallow caused the highest IRP to be 14.1 mm of Hg. So as per Chicago classification v 4.0 a diagnosis of “Distal Esophageal Spasm (DES)” was made and patient was put on calcium channel blockers with a repeat manometry planned after 6 months. However, there was no significant improvement in patients’ symptoms, rather the ECKARDT score worsened over one-month time (7 from 6 over one month). After discussion with the patient, option of Pneumatic Balloon Dilatation was opted, and LES was dilated with the pneumatic balloon of 30 mm with a pressure of up to 8 PSI. Patients’ symptoms improved with follow-up ECKARDT score of 1 after one month.
Discussion
There are a few case reports in the past suggesting the evolution of DES into Achalasia over a span of 9 months to 5 years and most of them used conventional manometry as a tool to measure the pressure changes with more chances of error [2-5]. High resolution manometry allows a much clear interpretation of topographic analysis of the data acquired during the study. The color hues indicating the pressures are capable of highlighting even the slightest changes with great accuracy making the differential diagnosis more confident.
Most of the case reports in the past have shown the change in pattern at two distant occasions separated over a time span. Even one case report that was High-Resolution Impedance Manometry (HRIM) based showed the change of pattern from DES to pan-esophageal pressurizations was over a span of 9 months [2]. To our knowledge our case is unique reporting the transition from DES to Achalasia pattern during one single study. While allowing the patient to have viscous swallows, the pattern not only changed from premature contractions to pan-esophageal pressurizations, but the IRP also started rising towards 15 mm of Hg.
DES may extend its affect towards LES involving the sphincter itself and raising its pressure, further creating difficulty in differentiating DES from Achalasia, however this can create a possible error amongst DES and type III Achalasia, where the topographic appearance of esophageal body is showing some peristaltic activity having premature contractions depicting a DL of < 4.5 seconds. Term “Vigorous Achalasia” is sometimes used for cases having overlapping properties of Achalasia and DES especially radiologically [6]. Chicago v4.0. have tried to address this issue by emphasizing on the number of premature contractions that is, the more you have premature contractions the more confidence you will have on the diagnosis of Type III Achalasia. Practically speaking in a true type III Achalasia there should be no peristaltic activity otherwise you are dealing with DES with Esophageal Gastric Junction Outlet Obstruction (EGJOO) [1]. In our case by the end of the study, the topographic pattern changed to pan-esophageal pressurizations, that is the feature of Type II achalasia.
Apart from DES, few more spastic motility conditions have also been reported in the literature that have evolved to Achalasia. Jason Abdallah and Ronnie Fass have reported a case of 66-year-old lady who presented with Jackhammer esophagus and over a span of 6 months evolved to Type II Achalasia [7]. Our case though showed a cork-screw pattern on barium swallow but none of the swallows met the criteria of hyper contractile esophagus. Although the treatment strategies for Achalasia and DES overlap, however special considerations have to be made while deciding for intervening patients with spastic esophageal motility disorders. Pharmacologic agents including calcium channel blockers even with Per-oral endoscopic Myotomy (POEM), the first line recommended technique for classic Achalasia, the results vary when applied to spastic disorders. For Type III Achalasia the success rate is about 92%, for DES its 88% and for hyper contractile esophagus its 72% respectively [8]. Furthermore, a much longer sub-mucosal tunnel is expected in spastic cases (16-18 cm) as compared to conventional cases (8-10 cm) [9,10].
Conclusion
In short, patients with DES may develop achalasia, particularly if their symptoms deteriorate over time, however this is less common than what has been suggested by previously published cases. The majority of DES patients maintain their manometric features throughout time; nevertheless, a sizeable portion of patients may see dysmotility worsening with little to no esophageal body motility, a hallmark of achalasia. Clinically and manometrically, DES is still an enigmatic concept. The association between various motility diseases can be further established by repeating High Resolution Manometry, however research must concentrate on the rate of advancement in people who have low amplitude esophageal contractions. A longer period of observation could help to determine the true rates of manometric development from DES to achalasia.
References
- Yadlapati R, Pandolfino JE, Fox MR, Bredenoord AJ, Kahrilas PJ, et al. What is new in Chicago Classification version 4.0?. Neurogastroenterol. Motil. 2021; 33: e14053.
- De Schepper HU, Smout AJ, Bredenoord AJ. Distal esophageal spasm evolving to achalasia in high resolution. Clin. Gastroenterol. Hepatol. 2014; 12: A25-26.
- Khatami SS, Khandwala F, Shay SS, Vaezi MF. Does diffuse esophageal spasm progress to achalasia? A prospective cohort study.Dig. Dis. Sci. 2005; 50: 1605–1610.
- Fontes LH, Herbella FA, Rodriguez TN, Trivino T, Farah JF, et al. Progression of diffuse esophageal spasm to achalasia: Incidence and predictive factors. Dis. Esophagus. 2013; 26: 470-474.
- Richter JE. The diagnosis and misdiagnosis of achalasia: It does not have to be so difficult. Clin. Gastroenterol. Hepatol. 2011; 9: 1010–1011.
- Jayabalan J, Theckumparampil N, Natarajan A, Phansalkar DS, Kurian G, et al. Vigorous achalasia: Zebra amongst horses. SA J. Radiol. 2020; 24: 1–4.
- Abdallah J, and Fass R. Progression of jackhammer esophagus to type II achalasia. J. Neurogastroenterol. Motil. 2016; 22: 153.
- Wong I, and Law S. Peroral endoscopic myotomy (POEM) for treating esophageal motility disorders. Ann. Transl. Med. 2017; 5: 1-8.
- Khan MA, Kumbhari V, Ngamruengphong S, Ismail A, Chen YI, et al. Is POEM the answer for management of spastic esophageal disorders? A systematic review and meta-analysis. Dig. Dis. Sci. 2017; 62: 35–34.
- Stavropoulos SN, Desilets DJ, Fuchs KH, Gostout CJ, Haber G, et al. Per-oral endoscopic myotomy white paper summary. Surg. Endosc. 2014; 28: 2005–2019.