
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Pott’s puffy tumor: A case report
N Birgach1*; M Attibbi1; K EL Fakiri1; N Rada1; G Draiss1; M Bouskraoui1; Y Rochdi2; H Nouri2 ; A Raji2; S Ouazzani3; S Belghmaidi3; I Hajji3; A Moutaouakil3
1Pediatric A Department, Mohammed VI University Hospital, Marrakech, Morocco.
2ORL and Cervico-Facial Department, Mohammed VI University Hospital, Marrakech, Morocco.
3Ophtalmology Department, Mohammed VI University Hospital, Marrakech, Morocco.
*Corresponding Author : N Birgach
Pediatric A Department, Mohammed VI University Hospital, Marrakech, Morocco.
Email: birgachnada@gmail.com
Received : Dec 26, 2022
Accepted : Jan 16, 2023
Published : Jan 23, 2023
Archived : www.jcimcr.org
Copyright : © Birgach N (2023).
Abstract
Pott’s puffy tumor is a subperiosteal abscess due to frontal osteomyelitis. It may occur in the setting of a local trauma or as a rare complication of frontal/ethmoid sinusitis.
We report the case of a 14-year-old boy, with no particular history and no recent trauma, who was admitted for headaches associated with a frontal and orbital swelling of inflammatory appearance. On workup, the child presented a hyperleukocytosis of 14210/ uL with a predominance of neutrophils at 9670/ uL and lymphocytes at 2730/ uL and a CRP of 157 mg/L. The cranioperitoneal CT scan showed pansinusitis complicated by Chandler stage 1 left orbital cellulitis, left frontal osteitis and homolateral cerebral empyema measuring 13.8 x 22 mm. Cytobacteriological examination yielded 6 cc of pus with a serum-like appearance and a gram-positive cocci in a chain-like pattern on direct examination. The patient was treated with triple antibiotic therapy with cipofloxacin, ceftriaxone and metronidazole for 21 days in IV and then relayed per os with ciprofloxacin for 6 weeks with good clinical evolution.
Early diagnosis and prompt treatment of this pathology is crucial to reduce the risk of developing endocranial complications such as meningitis, cerebral thrombophlebitis, empyema and brain abscess.
Citation: Birgach N, Attibbi M, EL Fakiri K, Rada N, Draiss G, et al. Pott’s puffy tumor: A case report. J Clin Images Med Case Rep. 2023; 4(1): 2253.
Background
Pott puffy tumor is a rare entity, characterized by the association of a subperiosteal abscess and osteomyelitis of the frontal bone. It is often secondary to frontal sinusitis or trauma. We report the case of a 14-year-old child who presented with a Pott’s tumor following frontal sinusitis, complicated by subdural empyema. He was successfully treated with antibiotic therapy and percutaneous drainage of the frontal abscess.
Observation
A 14-year-old patient presented to the pediatric A department for left orbital and frontal swelling evolving for 10 days, without any notion of trauma. The onset of the symptoms was marked by headaches and nasal congestion, complicated after 4 days left frontal and homolateral palpebral swelling. All evolving in a context of apyrexia.
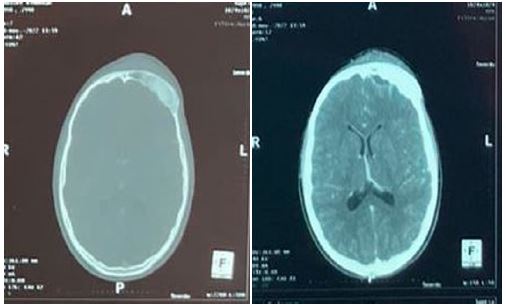
Clinical examination finds a patient who presents with hot and painful red palpebral and frontal tumefaction on palpaAbstract tion without damage to the oculomotor muscles or loss of visual acuity or neurological deficit with on rhinocavoscopy the presence of pus in the left middle meatus with on the biological assessment a hyperleukocytosis at 14,000 polymorphonuclear neutrophil with a CRP of 157. The hemoglobin and platelet counts were correct. Enhanced cerebro-orbital CT revealed pansinusitis complicated by left orbital cellulitis, left frontal osteitis and ipsilateral frontal cerebral empyema.

Percutaneous drainage of the abscess under the periosteum revealed gram-positive cocci in a chain. The patient was treated by ceftriaxone, ciprofloxacin and metronidazole for 21 days intraveinous then switched by ciprofloxacine orally for 6 weeks. Surgical treatment was not indicated at this stage. The evolution was marked by a decrease in the inflammatory swelling with the possibility of palpebral opening after one week.
Discussion
Pott’s puffy tumor, described by British surgeon Sir Percival Pott, is a polymicrobial infection that has become less common with adequate antibiotic treatment [1]. The term tumor refers to one of the 4 components of the inflammation (tumor) and not neoplasia [1]. Although it may be secondary to head trauma, it generally occurs following untreated or poorly treated frontal sinusitis [1,4,5]. This pathology is frequently seen in patients between 6-15 with a male predominance [1], due to increased vascularization and growth of the frontal sinuses at this age [4,1].
Frontal sinusitis can have intra and extra cranial complications following hematogenous dissemination, through the rich diploic venous networks and septic embolism [1,3,5,6], or the direct extension of infection, through the posterior wall causing epidural/subdural empyema, brain abscess, or meningitis, through the anterior wall causing subperiosteal abscess, or through the inferior wall with orbital complications [1-3,5,6]. Note that the most common orbital complications, occurring in 29% of cases, are preseptal and periorbital cellulitis. However, intraorbital abscesses are very rare [2].
The most common clinical signs are forehead swelling, headache, fever, nasal congestion or purulent/non-purulent secretions [1,4,5]. A soft, erythematous forehead swelling associated with fever is considered pathognomonic for Pott’s tumour [1]. In some cases fever may be absent, and other signs may be associated including orbital swelling, nausea/vomiting and meningeal syndrome [1].
In our case, the patient presented to the emergency department for two frontal and orbital swellings with a history of headaches and nasal congestion. Fever was absent in our setting. He subsequently benefited from an injected cerebral-ocular CT scan, although MRI remains the examination of choice with its high soft tissue resolution, best characterizing the extent of the infection [1,5,6]. CT showed pansinusitis complicated by osfrontal osteomyelitis, frontal lobe empyema and preseptal cellulitis.
The literature has confirmed that intracranial complications, with or without bone erosion, have been observed in 60% to 85% of cases [5,6,9,10] and may be asymptomatic until late in their evolution, especially when “silent” areas of the central nervous system such as the frontal lobe are involved [6].
The most common microorganisms are non-enterococci streptococci (47%), anaerobic bacteria (28%), staphylococci (22%) [1]. In our case, the culture was sterile, but direct examination revealed objective a gram positive cocci in chain.
The management of swollen pott’s tumor is multidisciplinary; it consists of medical treatment, with broad-spectrum antibiotic therapy administered intraveinous as soon as possible. The combination of ceftriaxone and clindamycin can be used to treat frontal sinusitis. In the case of Staphylococcus aureus (MRSA) which is generally resistant to clindamycin, vancomycin should be used in addition to ceftriaxone. Combination therapy with vancomycin, ceftriaxone, and metronidazole covers most intracranial pathogens complicating acute bacterial sinusitis. In this case, metronidazole was chosen to be added to ceftriaxone and ciprofloxacin initially because of his good diffusion in the bones. A previous study showed that sinus related intracranial epidural abscesses in children could be managed without neurosurgical procedures in the setting of adequate sinus drainage, appropriate antibiotic therapy and minimal extradural mass effect from the abscess [11].
Conclusion
Although rare, Pott’s tumor, frontal osteomyelitis, is a severe complication of frontal sinusitis. It can still occur despite the use of antibiotics and requires surgical treatment with drainage of the abscess and filling of the frontal sinus with different materials. It rarely progresses to intracranial extension potentially fatal.
References
- Jose I Sandoval. Orlando De Jesus: Pott Puffy Tumor. StatPearls Publishing. 2022. Last Update: August 29, 2022 NBK560789
- Elif Gozgec, Hayri Ogul, and Korhan Kılıc:Pott’s Puffy Tumor with Intraorbital Abscess.Rev Soc Bras Med Too. 2022; 55: e0126-2022. 10.1590/0037-8682-0126-2022
- Liliana Costa, Laurentino Mendes Leal, Fernando Vales, and Margarida Santos: Pott’s edematous tumor: Rar a complicação da sinusitis. Braz J Otorhinolaryngol. 2020; 86: 812–814. 10.1016/j.bjorl.2016.08.005
- Song MW, Montovano M, Kubiak A, et al. Pott’s Puffy Tumor: Intracranial Extension Not Requiring Neurosurgical Intervention. Cureus. 12: e10106.10.7759/cureus.10106
- Pranav Sharma,Salil Sharma,Nishant Gupta,Puneet Kochar, andYogesh Kumar: Pott puffy tumor.Proc (Bayl University Med Cent). 2017; 30: 179–181.
- İbrahim Ketenci, Yaşar Ünlü, Bülent Tucer, Alperen Vural. The Pott’s puffy tumor: A dangerous sign for intracranial complications. European Archives of Oto-Rhino-Laryngology. 2011; 268: 1755–1763. 10.1007/s00405-011-1660-5
- Adetunji Adejumo, Olusegun Ogunlesi, Ameera Siddiqui, Vel Sivapalan, Oladipo Alao, et al. Pott Puffy Tumor Complicating Frontal Sinusitis. The american journal of the medical sciences. 2010; 340: 79. 10: 1097/MAJ.0b013e3181bdb5b5
- Rachel Tattersall, Prof Robert Tattersall. Pott’s puffy tumor. The lancet. 2002; 359: 989-1078. 10.1016/S0140-6736(02)08098-4.