
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Massive rectal bleeding caused by diversion colitis
Seung Min Hong; Dong Hoon Baek*; Geun AM Song
Division of Gastroenterology, Department of Internal Medicine, Pusan National University School of Medicine and Biomedical Research Institute, Pusan National University Hospital, South Korea.
*Corresponding Author : Dong Hoon Baek, MD
Department of Gastroenterology, Pusan National University School of Medicine and Biomedical Research Institute, Pusan National University Hospital, 179, Gudeok-ro, Seo-Gu, Busan, 49421, South Korea.
Tel: +82-51-240-7869, Fax: +82-51-244-8180;
Email: dhbeak77@gmail.com
Received : Dec 29, 2022
Accepted : Jan 17, 2023
Published : Jan 24, 2023
Archived : www.jcimcr.org
Copyright : © Baek DH (2023).
Citation: Hong SM, Baek DH, Song GA, et al. Massive rectal bleeding caused by diversion colitis. J Clin Images Med Case Rep. 2023; 4(1): 2255.
Description
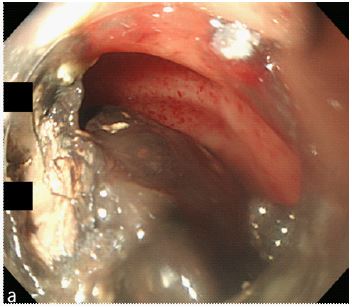
A 74-year-old male patient presented to the emergency department with hematochezia and dizziness. Seven years ago, the patient had a colonoscopy at another hospital, during which a perforation in the sigmoid colon was found; consequently, he underwent a loop colostomy. He was pale, with a blood pressure of 70/40 mmHg and a pulse of 130 beats per minute. Laboratory evaluation revealed a hemoglobin level of 8.3 g/dL, platelets of 280,000/mm3. An abdomen and pelvis computed tomography scan revealed contrast leakage into the rectum (Figure 1). Emergent sigmoidos copy revealed a huge dark grey mucous stool (Figure 2a) and a 5 mm sized bleeding vessel with an adherent clot within a field of shallow ulceration near the anal verge (Figure 2b). The large protruding vessel with adherent clot was treated with thermal coagulation. The mucous stools were fragmented and removed using forcep, endoscopic polypectomy snare and Roth Net retriever (Figure 2c). There had been no recurrence of bleeding after 12 months of follow-up (Figure 2d).
Diversion colitis, also referred to as bypass or disuse colitis, is defined as a nonspecific inflammation of the large intestine following surgical diversion of the fecal stream away from the upstream colon. Diversion of the fecal stream results in a deficiency of short-chain fatty acids and other luminal nutrients in colonocytes in the diverted segment of the colon. It is hypothesized that the lack of these compounds or interference with their metabolism by alterations in gut flora may have a role in the development of colitis [1]. Diversion colitis is more common in patients with underlying inflammatory bowel disease (ie, Crohn disease and ulcerative colitis) than those with malignancy and diverticular diseases. Since diversion colitis is usually asymptomatic, it often results in late diagnosis. Furthermore, its symptoms, which include lower abdominal pain, pelvic pain, and tenesmus, are often similar to those of other types of enterocolitis [2]. Although massive rectal bleeding caused by diversion colitis that require blood transfusion are known to be rare, it should be considered in the differential diagnosis of hematochezia for patients to whom reconstruction is not an option [3]. For patients to whom reconstruction is not an option, regular follow-up is needed.

Declarations
Written informed consents were obtained.
Conflict of interest: No potential conflict of interest relevant to this article was reported.
References
- Harig JM, Soergel KH, Komorowski RA, Wood CM. Treatment of diversion colitis with short-chain-fatty acid irrigation. N Engl J Med. 1989; 320: 23-28.
- Haas PA, Fox TA, Jr., Szilagy EJ. Endoscopic examination of the colon and rectum distal to a colostomy. Am J Gastroenterol. 1990; 85: 850-854.
- Whelan RL, Abramson D, Kim DS, Hashmi HF. Diversion colitis. A prospective study. Surg Endosc. 1994; 8: 19-24.