
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
LESS score and isometric lower limb strength after ACL reconstruction in female handball players
Razvan Marian Melinte1,2,3,4; Adrian Blesneac1; Ovidiu Aurelian Budisca5*; Dan Nicolae Zolog-Schiopea1,2; Gabriel Koszorus4; Dan Avramiuc4; Adrian Dumitru Ivănescu6; Marian Andrei Melinte7; Emil Marian Arbanași8,9,10; Mircea Tabacar1,4
11Puls Hospital of Regina Maria Hospital, Targu Mures, Romania.
22Humanitas Hospital, ClujNapoca, Romania.
33Dimitrie Cantemir University, Targu Mures, Romania.
44Mures County Emergency Hospital, 540136, Targu Mures, Romania.
55Department of Surgery, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Targu Mures, 540139, Targu Mures, Romania.
66Department of Anatomy, George Emil Palade University of Medicine, Pharmacy, Sciences and Technology of Targu Mures, 540139, Targu Mures, Romania.
77Faculty of Medicine, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Targu Mures, 540139, Targu Mures, Romania.
88Clinic of Vascular Surgery, Mures County Emergency Hospital, 540136, Targu Mures, Romania.
99Department of Vascular Surgery, George Emil Palade University of Medicine, Pharmacy, Science, and Tech-nology of TarguMures, 540139, Targu Mures, Romania.
1010Doctoral School of Medicine and Pharmacy, George Emil Palade University of Medicine, Pharmacy, Sciences and Technology of Targu Mures, 540142, Targu Mures, Romania.
*Corresponding Author : Ovidiu Aurelian Budișca
Department of Surgery, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Targu Mures, 540139, Targu Mures, Romania.
Email: ovidiu.budisca@umfst.ro
Received : Dec 28, 2022
Accepted : Jan 18, 2023
Published : Jan 25, 2023
Archived : www.jcimcr.org
Copyright : © Budisca OA (2023).
Abstract
Background: Anterior Cruciate Ligament (ACL) injuries have amplified dramatically in the last years in female team sports due to the incrementing number of teams and players, an increase in speed and competitivity, and in some areas due to insufficient strength training in young athletes. Return to play is main goal after ACL reconstruction. Access to surgery and rehabilitation is mandatory for an successful return to sport after the injury;
Methods: We analysed a sample of high-performance female athletes with ACL tears, all professional sport athletes, after surgery and during the rehabilitation process, to determine more specific returning to sport criteria based on the relation between the Landing Error Score System (LESS) and isometric limb strength measurements. Returning to sports and returning to play are the most difficult challenges after an ACL injury, requiring a long rehabilitation period, with multiple possible reasons for graft failure.
Results: The force-to-weight ratio of all dynamic stabilizers of pelvis and knee, both in the frontal and sagittal planes, significantly improved between the two testing sessions as follows: Flexion of the operated limb +0.78 N/kg (SD=1.022, p=0.0061), Extension of the operated limb +1.65 N/kg (SD=1.618, p=0.0003), Adduction +1.77 N/kg (SD=2.021, p=0.0012), Abduction +1.33 N/kg (SD=2.069, p=0.0120). We also found a significant reduction in the difference in isometric muscle strength between the operated limb and the contralateral limb before and after the rehabilitation protocol, with a value of -37 N for flexion (±5.54, p< 0.0001) and a value of -76.77 N for extension (±20.68, p=0.0016). The LESS Score significantly diminished between the two sessions by 6 points on average. (p< 0.0001).
Conclusions: The LESS Score and isometric muscle strength measurements are complementary to each other and useful in accurately describing the patient’s status who benefited from a well-conducted rehabilitation program, by diminishing the dynamic valgus, the abnormal knee kinetics and kinematics, and their deleterious effects and in assessing the readiness for return to play together with complimentary criteria in female team sport.
Keywords: Anterior cruciate ligament reconstruction; ACL; Isokinetic strength; Female athletes; Less score; Handball; Return to play.
Citation:Melinte RM, Blesneac A, Budișcă OA, Zolog-Schiopea DN, Koszorus G, et al. LESS score and isometric lower limb strength after ACL reconstruction in female handball players. J Clin Images Med Case Rep. 2023; 4(1): 2257.
Introduction
Non contact injuries represent the most frequent mechanism involved in Anterior Cruciate Ligament (ACL) lesions in female athletes participating in an contact team sport like handball, basketball, lacrosse. These usually occur during abrupt deceleration, landing, or lateral pivoting, with the involvement of underlying chronic fatigue, hormonal variation, familial factors [1–4,47].
Dynamic Knee Valgus (DKV) is a combination of hip adduction, internal rotation, and abduction of the knee. This is one of the most frequently involved patterns in non-contact ACL injuries and re –injuries in landings or high speed cutting and although many studies have shown the DKV importance regarding injury prevention and return-to-sport, it is still difficult to quantify the extent of this condition [3,5-10].
Female athletes are more prone to this specific type of injury, because of various factors including biomechanical (larger pelvic width, increased Q angles) and hormonal factors (lower testosterone levels, increased hormonal-induced muscle inhibitions in the first 12-16 months after birth or during the luteal phase of the menstrual cycle) [6,10-12].
The decision to return to sport after ACL reconstruction surgery is complex, and multifactorial and comprises biological, biomechanical, and psychosocial factors. Thus far no consensus, well-established criteria or clear guidelines exist in the literature to guide the process but recent studies show that delaying it reduces the re injury rate [13-19].
Is okinetic testing represents an objective way to assess muscle strength and along-side various functional testing (single leg hop, cross-over hop, triple hop, shuttle run, carioca test, Landing Error Scoring System - LESS) [20,21]. may be used to evaluate the dynamic stability of the knee correlated with isokinetic strength of main muscle groups. The aim of our study is to evaluate the strength of the muscles involved in the dynamic stability of the knee, pelvic abductors and adductors and knee flexors and ex-tensors, after ACL reconstruction and rehabilitation in professional female handball players through is okinetic and functional testing for determining the readiness for contact sport reintegration.
Materials and methods
Study design
After ACL reconstruction surgery, all or athletes underwent a specific rehabilitation program focused on protecting the joint, restoring range of motion, obtain static strength and stability and finally good plyometric qualities for reintegrating the athlete in a ballistic contact sport. During the rehabilitation process we tested the athlete on the Easy Torque device for is okinetic strength of main muscle groups – pelvic stabilizers [hip adductors and abductors] and knee flexor and extensors, at 12-16 weeks and 24 after surgery and during same test session LESS test was performed as described further. The main objective was to correlate the growth of isokinetic force [maximal value and specific value strength/body weight] with the diminishing of the LESS score [the lower the better -meaning lower value show good knee hip/knee/ankle stability during landings and no dynamic knee valgus] because horizontal hop tests alone are not as specific in determining the return to play after ACL surgery and we consider that time after surgery is not an criteria [ 9,42].
Data collection
We examined, operated on, and followed during the rehabilitation process until return to play a group of 28 professional female handball players, aged 18 to 34, who sustained a non-contact sports injury resulting in an ACL rupture. All the subjects playing at the time of injury in the Romanian National Women’s Handball League were of different nationalities – Romanians, Brazilians, Serbians, Spaniards, and Byelorussians – and members of their respective national handball teams. The diagnosis was made after a thorough examination of the mechanism of injury, which was very typical and caught on live TV, clinical examination, knee radiographs, MRIs, and con-firmed arthroscopically at the time of definitive surgery.
Test Data collection from Easy Torque device after testing was in specific patient named folder with printing of individual results, statistic analysis was made on this data, same electronic measurement machine Easy Torque with specific and individual inputs [sex, age, bodyweights] make data acquisition and measurements reliable and accurate. LESS test was recorded on camera and data and measurements were made electronically by the same group of authors with marginal error possible as on all HOP and Landing Tests.
Exclusion and inclusion criteria
Exclusion criteria were multiple ligament injuries – 1, unstable meniscal tears – 3, bony deformities – increased posterior tibial slope – 1, genu varum/valgus more than 5 degrees – 1, severe flatfoot – 1, ipsilateral previous knee surgery – 2. After exclusion, 19 patients were included in our study. The study was conducted between January 2019 and December 2022.
All patients signed informed consents and participated willingly in our studies. Approval from the ethical commissions of the rehabilitation facility and the clinical hospital was obtained.
ACL reconstruction surgery
All patients underwent 2-4 weeks of prehab. The surgery was performed by the same senior surgeon carrying out more than 150 ACL reconstructions/per year. Standard arthroscopic reconstruction of the ACL was carried, out using a quadrupled Semitendinosus and Gracilis graft used in all cases [22]. All grafts below 7 mm in diameter were braided in order to increase the diameter and tensile strength, while grafts between 7 mm and 8 mm were reinforced using Fiber Tape, an ultra-high-strength non-absorbable suture (Arthrex, Naples, Florida, USA) – so final diameter of all grafts was over 8 mm. Femoral cortical fixation was achieved using an adjustable loop but-ton, ACL Tight Rope II (Arthrex, Naples, Florida, USA), while bioresorbable interference screws were utilized for tibial fixation of the graft (Arthrex, Naples, Florida, USA), doubled in some cases by a titanium staple.
Rehabilitation protocol
All patients were allowed to weight-bear as tolerated immediately after surgery and the postoperative rehabilitation protocol commenced the first day after surgery with cvadriceps contractions, hip and ankle mobility exercises, with an extension orthosis used 7-10 days after surgery. The rehabilitation program was focused on achieving dynamic knee stability and was based but not limited on practice guidelines provided by van Melick et al [23].
After protection phase the goal was to obtain full range of motion, decrease swelling, improve muscle strength, slowly isometric exercises were developed into eccentric strength exercises, stability and proprioception exercises with focus on knee stability.at and after 12-14 weeks strength training for lower limb was introduced in all cases and progressing to light running and plyometric training with and without external perturbations was started at 16-18 weeks depending of individual tolerability. Normal Range of Motion and absence of knee effusion was considered mandatory for progressing to running and plyometric training.
Return to sport and consequently return to play was allowed after passing the second test with normal LESS, limb symmetry index of more than 90% on strength measurement and horizontal hop test -single-triple- of more than 90 % compared to contralateral leg.
Study outcomes
We measured and analysed isometric muscle forces on the Easy Torque machine (TONUS sports & reha GmbH, Zemmer, Germany). The tests were performed in two sessions, the first one at 12-16 weeks after surgery and the second 24-26 weeks after surgery before finalizing the rehabilitation protocol and reintegration in team activity.
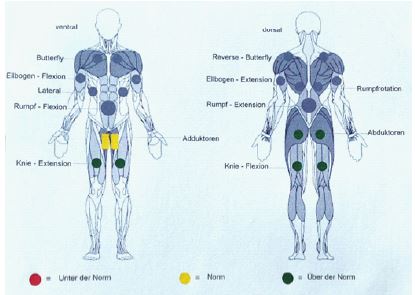
The testing procedure was modified after the one described by Cvjetkovic et al [24] as following: each patient performed a 6 minute active warm-up; they were tested in a seated position (Figures 1); both limbs were tested simultaneous; for the sagittal plane movement, the range of motion of the knee joint was from 0° to 90°; adduction and abduction were measured without restricting the range of motion; all tests were performed three times with a two minute rest period between the tests; vocal encouragement was performed systematically; The maximum value of each parameter (flexion, extension, abduction and adduction) were considered and compared with the reference values which were calculated based on the Easy Torque machine software, taking into account gender, age, weight and height; The force-to-weight ratio for each movement was also calculated (Figure 2).
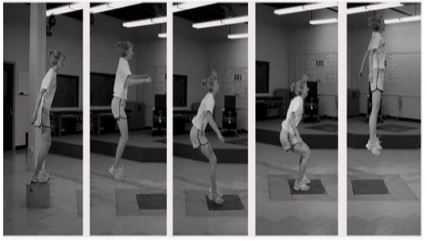
During the same testing sessions, the LESS was also performed as described by Padua et al (Figure 3) [21]. The subjects were filmed from two angles while performing a drop-vertical jump from a 30 cm box to a distance of one half of their height, followed by a maximal vertical jump. The two videos were then analysed and the LESS calculated. Improvement of LESS score shows a reducing of the score because being a Landing Error Score a number is attributed to each error, so the lower the score the better and the more stable landing and knee we have.

Statistical analysis
The statistical analysis was performed using Prism 9 for Windows, Version 9.4.1 (681), GraphPad Software, LLC. And results are displayed below.
Results
CThe maximum strength of all parameters which were measured during the first testing session was above the reference values in 92.1% of the cases and twice above the reference values in 27.2% of all cases which represent very good values for the same gender and age group.
The average time elapsed between the two testing sessions was minimum 56 days maximum 72 days.
The force-to-weight ratio of all dynamic stabilizers of the knee, both in the frontal and sagittal planes, significantly improved between the two testing sessions as follows: Flexion of the operated limb +0.78 N/kg (SD=1.022, p=0.0061), Extension of the operated limb +1.65 N/kg (SD=1.618, p=0.0003), Adduction +1.77 N/kg (SD=2.021, p=0.0012), Abduction +1.33 N/kg (SD=2.069, p=0.0120), all represented in Figure 4.
Absolute strength and individual muscle group strength is one of the main contributor to knee injury prevention in female athletes [9,43-44].
The LESS Score significantly diminished between the two sessions by 6 points on average (p< 0.0001) (Figure 5).


We found a direct between the LESS scores improvement [lower score number] and the measured muscle isometric strength parameters which shows that knee stability is improving both through the direct implication of analysed muscle groups in stabilization of knee and through the plyometric and proprioceptive rehabilitation specific training. In our group of players at 24 months we had no Return to Play before 32 weeks and we had no ACL reinjury or contralateral ACL Injury at 24 months after surgery.
Discussion
Return To Play (RTP) and Return To Sport (RTS) are the main objectives of professional athletes after technically successful surgery, with rates of returning to competitive sports varying between 55% and 83% [25,26]. Pressure on Team Player, Doctor and Physical Trainer or Physio therapist’ is mounting as time after surgery goes by and reaches a summit in the return to specifically functional training during the athletes team re integration. Patient re-education and appropriate exercise-based rehabilitation protocols are the cornerstones of postoperative management after ACL reconstruction. The rehabilitation protocol should include weight-bearing, mobility, open and closed kinetic chain resistance-based neuromuscular control, and plyometric exercises [27]. Achieving pre trauma muscle strength is mandatory and comparing the operated limb to the non operating limb considered as individual golden standard is the only option we have .In order to achieve this, we consider that for female athletes the optimum timeframe to RTP is closer to 10 months considering that the ligamentisation process of the graft takes much longer than previously believed [45].
In order to clear an athlete to RTP, multiple factors should be considered, including body composition, aerobic fitness levels, and psychological readiness, along with passing the various tests for evaluating the dynamic stability of the knee criteria (Limb Symmetry Index, Vertical and Horizontal Hop Tests, isometric and Isokinetic Strength Tests, LESS). These are complementary to each other, with the literature suggesting a low to moderate correlation between tests and muscle strength measurements in patients who underwent ACL reconstruction [28]. These are the reason why multiple criteria should be used.
Horizontal and vertical Hop tests remain important tools in assessing the functional outcomes after ACL reconstruction, and alongside muscle power output measurements are useful in comparing the operated limb with the contralateral one – in our opinion, there should be a minimum of 95% symmetry.
Pressure on professional athletes to achieve an early RTP (under six months) re-mains elevated because of various factors – contract renewal, maintaining a first-team place, sustaining their status, the eligibility to be selected for the national team’s roster in order to participate in one of the numerous competitions which take place regularly – European Championships, World Cup, Olympics.
However, six months after the initial surgery, most of the athletes are not pre-pared for RTP, with few passing the majority of the proposed RTS criteria. There is conclusive evidence to wait at least nine months until returning to pre-injury sports, a study by Bodkin et al. showing that second ACL reinjury risk was diminished by 28% for every month that RTP was delayed beyond 8 months [29].
MRI evaluation of the integration of the graft should also be considered [30-32]. Although the development of surgical techniques and improved rehabilitation protocols have been remarkable, the repercussions of an ACL injury are still significant. The average length of the professional career of an athlete who underwent ACL surgery is diminished when comparing it to uninjured athletes, and it is accompanied by de-creased performance and less playing time [33-36].
The reinjury rates in the first months after RTP are especially high in female athletes [37-39]. A second injury on the contralateral leg is also to be considered [19,29]. The prevalence of secondary osteoarthritis after primary ACL surgery, as well as revision surgery, remains high [37,40,41].
Contralateral ACL injury is an event which occurs also often in the first two years after surgery and should be considered [46].
The authors observed through consecutive testing’s on Easy Torque after Return To Play that actually during the first 6 months team playing, the absolute muscle strength measured on isokinetic machine diminishes probably due to fatigue, aerobic and plyometric or functional sport training and lack of strength training because of team schedule and coach preferences .also being integrated in a team make it more difficult for a handball player to maintain a individual strength program than for an individual sport athlete.
Conclusion
We conclude that in the absence of a golden standard of RTP criteria, the LESS Score and isometric muscle strength measurements are complementary to each other and useful in accurately describing the patient’s status who benefited from a well-conducted rehabilitation program, by diminishing the dynamic valgus, the abnormal knee kinetics and kinematics, and their deleterious effects. We consider that in the return to play criteria time after surgery should be measured in favour of the athlete as, as we showed the longer the rehabilitation the better the maturation of the graft, the lower the reinjury risk is.
Women Handball is a sport with a very high rate of ACL injury and reinjury, it is a very fast stop and go contact sport in which deceleration, pivoting, cutting an landing is producing an high amount of forces on an athlete’s knee which is especially after an ACL surgery prone to re injury. Aerobic capacity and psychological readiness should always be considered individually.
Although recent advances in surgical technique and rehabilitation protocols are notable, the reinjury rate persists and an SACL re-injury is an devastating event for the carrier of an team athlete.
Time is not on the patient’s side an is something which is always forgotten, a hasty recovery process should be avoided because it leads to more injuries and reinjuries, and elapsed time from the index surgery should not be considered as an RTP factor on its own but should be considered when approaching the recovery process.
Declarations
Author contributions: Conceptualization, methodology, writing—original draft preparation, R.M.M., M.T.; software, A.B., O.A.B., D.N.Z-S.; formal analysis, investigation, G.K.; resources, D.A., A.D.I.; writing—review and editing, E.M.A., R.M.M.; data curation, project administration, visualization, supervision, M.T.; validation, all authors. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Institutional review board statement: The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Fizionova Sports Clinic, Targu Mures Romania (protocol code 3, on 01 December 2022) and Ethics Committee of Regina Maria Health Network Targu Mures, Romania (protocol code 202, on 02.09.2022).
Informed consent statement: Informed consent was obtained from all subjects involved in the study.
Data availability statement: Not applicable.
Acknowledgments: We would like to thank all participants for their support and approval of this paper.
Conflicts of interest: The authors declare no conflict of interest.
References
- Besier TF, Lloyd DG, Ackland TR. Muscle Activation Strategies at the Knee during Running and Cutting Maneuvers. Med. Sci. Sports Exerc. 2003; 35: 119–127.
- Shultz SJ, Schmitz RJ, Benjaminse A, Chaudhari AM, Collins M, et al. ACL Research Retreat VI: An Update on ACL Injury Risk and Prevention. J. Athl. Train. 2012; 47: 591–603.
- Kobayashi H, Kanamura T, Koshida S, Miyashita K, Okado T, et al. Mechanisms of the Anterior Cru-ciate Ligament Injury in Sports Activities: A Twenty-Year Clinical Research of 1,700 Athletes. J. Sport. Sci. Med. 2010; 9: 669–675.
- Weiss K, Whatman C. Biomechanics Associated with Patellofemoral Pain and ACL Injuries in Sports. Sport. Med. 2015; 45: 1325–1337.
- Toor AS, Limpisvasti O, Ihn HE, McGarry MH, Banffy M, et al. The Significant Effect of the Medial Hamstrings on Dynamic Knee Stability. Knee Surgery, Sport. Traumatol. Arthrosc. 2019; 27: 2608–2616.
- Asaeda M, Nakamae A, Hirat K, Kono Y, Uenishi H. et al. Factors Associated with Dynamic Knee Valgus Angle during Single-Leg Forward Landing in Patients after Anterior Cruciate Ligament Reconstruction. Asia-Pacific J. Sport. Med. Arthrosc. Rehabil. Technol. 2020; 22: 56–61.
- Hewett TE, Myer GD, Ford KR, Heidt RS, Colosimo AJ, Et al. Biomechanical Measures of Neuromuscular Control and Valgus Loading of the Knee Predict Anterior Cruciate Ligament Injury Risk in Female Athletes: A Prospective Study. Am. J. Sports Med. 2005; 33: 492–501.
- Tamura A, Akasaka K, Otsudo T, Shiozawa J, Toda Y, et al. Dynamic Knee Valgus Alignment Influences Impact Attenuation in the Lower Extremity during the Deceleration Phase of a Single-Leg Landing. PLoS One 2017; 12: 1–12.
- Melinte Razvan M, Koszorus G, Melinte Marian A, Papp E, Tabacar M, et al. D. Dynamic Knee Valgus in Anterior Cruciate Ligament Non-Contact Injury and Reinjury in Professional Female Athletes. Determinant or Not? J. Nov. Physiother. Rehabil. 2022; 6: 029–033.
- Wilczyński B, Zorena K, Ślęzak D. Dynamic Knee Valgus in Single-Leg Movement Tasks. Potentially Modifiable Factors and Exercise Training Options. a Literature Review. Int. J. Environ. Res. Public Health 2020; 17: 1–17.
- Constantini NW, Dubnov G, Lebrun CM. The Menstrual Cycle and Sport Performance. Clin. Sports Med. 2005; 24: 51–82.
- Mansouri R, Bahrami F, Rajabi R, Minoonejad H, Kaczmarczyk K. Investigating the Landing Kinetics Factors and Pre-paratory Knee Muscle Activation in Female Handball Players with and without Dynamic Knee Valgus While Performing Single Leg Landing. Biomed. Hum. Kinet. 2021; 13: 155–162.
- Webster KE, Feller JA. A Research Update on the State of Play for Return to Sport after Anterior Cruciate Ligament Re-construction. J. Orthop. Traumatol. 2019; 20: 10.
- Zhou L, Xu Y, Zhang J, Guo L, Zhou T, et al. Multiplanar Knee Kinematics-Based Test Battery Helpfully Guide Return-to-Sports Decision-Making after Anterior Cruciate Ligament Reconstruction. Front. Bioeng. Biotechnol. 2022; 10: 1–9.
- Filbay SR, Grindem H. Evidence-Based Recommendations for the Management of Anterior Cruciate Ligament (ACL) Rupture. Best Pract. Res. Clin. Rheumatol. 2019; 33: 33–47.
- Burland JP, Toonstra J, Werner JL, Mattacola CG, Howell DM, et al. Decision to Return to Sport after Anterior Cruciate Ligament Reconstruction, Part I: A Qualitative Investigation of Psychosocial Factors. J. Athl. Train. 2018; 53: 452–463.
- Meredith SJ, Rauer T, Chmielewski TL, Fink C, Diermeier T, et al. Return to Sport After Anterior Cruciate Ligament Injury: Panther Symposium ACL Injury Return to Sport Consensus Group. Orthop. J. Sport. Med. 2020; 8: 1–11.
- Sanborn RM, Badger GJ, Yen YM, Murray MM, Christino MA, et al. Psychological Readiness to Return to Sport at 6 Months Is Higher After Bridge-Enhanced ACL Restoration Than Autograft ACL Reconstruction: Results of a Prospective Randomized Clinical Trial. Orthop. J. Sport. Med. 2022; 10: 1–10.
- Wiggins ME, Fadale P, Barrach H, Ehrlich M, W.W. Risk of Secondary Injury in Younger Athletes after Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-Analysis. Am J Sport. Med 2016; 44: 1861–1876.
- Abrams GD, Harris JD, Gupta AK, McCormick FM ,Bush-Joseph CA, et al. Functional Performance Testing after Anterior Cruciate Ligament Reconstruction: A Systematic Review. Orthop. J. Sport. Med. 2014; 2: 1–10.
- Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE. The Landing Error Scoring System (LESS) Is a Valid and Reliable Clinical Assessment Tool of Jump-Landing Biomechanics: The Jump-ACL Study. Am. J. Sports Med. 2009; 37: 1996–2002.
- Valoroso M, Demey G, G Ntagiopoulos P, Dejour D. Arthroscopic Anterior Cruciate Ligament Reconstruction with Hamstring Tendons. In Arthroscopy; Springer Berlin Heidelberg: Berlin, Heidelberg, 2016; 229–237.
- Van Melick N, Van Cingel REH, Brooijmans F, Neeter C, Van Tienen T, et al. Evidence-Based Clinical Practice Update: Practice Guidelines for Anterior Cruciate Ligament Rehabilitation Based on a Sys-tematic Review and Multidisciplinary Consensus. Br. J. Sports Med. 2016; 50: 1506–1515,
- Cvjetkovic DD, Bijeljac S, Palija S, Talic G, Radulovic TN, et al. Isokinetic Testing in Eval-uation Rehabilitation Outcome After ACL Reconstruction. Med. Arch. (Sarajevo, Bosnia Herzegovina) 2015; 69: 21–23.
- Ardern CL, Taylor NF, Feller JA, Webster KE. Fifty-Five per Cent Return to Competitive Sport Following Anterior Cruciate Ligament Reconstruction Surgery: An Updated Systematic Review and Meta-Analysis Including Aspects of Physical Functioning and Contextual Factors. Br. J. Sports Med. 2014; 48: 1543–1552.
- Lai CCH, Ardern CL, Feller JA,Webster KE. Eighty-Three per Cent of Elite Athletes Return to Preinjury Sport after Anterior Cruciate Ligament Reconstruction: A Systematic Review with Meta-Analysis of Return to Sport Rates, Graft Rupture Rates and Performance Outcomes. Br. J. Sports Med. 2018; 52: 128–138.
- Whittaker JL, Culvenor AG, Juhl CB, Berg B, Bricca A, et al. OPTIKNEE 2022: Consensus Recommendations to Optimise Knee Health after Traumatic Knee Injury to Prevent Osteo-arthritis. Br. J. Sports Med. 2022; 0: bjsports-2022-106299.
- Fitzgerald GK, Lephart SM, Hwang JH, Wainner MRS. Hop Tests as Predictors of Dynamic Knee Stability. J. Orthop. Sports Phys. Ther. 2001; 31: 588–597.
- Bodkin SG, Hertel J, Diduch DR. Saliba SA, Novicoff WM, et al. Redicting Anterior Cruciate Ligament Reinjury From Return-to-Activity Assessments at 6 Months Postsurgery: A Prospective Cohort Study J. Athl. Train. 2022; 57: 325–333.
- Putnis SE, Klasan A, Oshima T, Grasso S, Neri T, et al. Magnetic Resonance Imaging Assessment of Hamstring Graft Healing and Integration 1 and Minimum 2 Years after ACL Reconstruction. Am J. Sports Med. 2022; 50: 2102–2110.
- Marchiori G, Cassiolas G, Berni M, Grassi A, Dal Fabbro G, et al. A Com-prehensive Framework to Evaluate the Effects of Anterior Cruciate Ligament Injury and Reconstruction on Graft and Cartilage Status through the Analysis of MRI T2 Relaxation Time and Knee Laxity: A Pilot Study. Life. 2021; 11: 1383.
- Figueroa D, Melean P, Calva R, Vaisman A, Zilleruelo N, et al. Magnetic Resonance Imaging Evalu-ation of the Integration and Maturation of Semitendinosus-Gracilis Graft in Anterior Cruciate Ligament Reconstruction Using Autologous Platelet Concentrate. Arthrosc. J. Arthrosc. Relat. Surg. 2010; 26: 1318–1325.
- Barth KA, Lawton CD, Touhey DC, Selley RS, Li DD, et al. Negative Impact of Anterior Cruciate Ligament Reconstruction in Professional Male Footballers. Knee. 2019; 26: 142–148.
- Read CR, Aune KT, Cain EL, Fleisig GS. Return to Play and Decreased Performance After Anterior Cruciate Ligament Reconstruction in National Football League Defensive Players. Am. J. Sports Med. 2017; 45: 1815–1821.
- Longstaffe R, Leiter J, Mac Donald P. Anterior Cruciate Ligament Injuries in the National Hockey League. Clin J. Sport Med. 2018.
- Buerba RA, Zaffagnini S, Kuroda R, Musahl V. ACL Reconstruction in the Professional or Elite Athlete: State of the Art. J. ISAKOS. 2021; 6: 226–236.
- Friel NA, Chu CR. The Role of ACL Injury in the Development of Posttraumatic Knee Osteoarthritis. Clin. Sports Med. 2013; 32: 1–12.
- Lohmander LS, Östenberg A, Englund M, Roos H. High Prevalence of Knee Osteoarthritis, Pain, and Functional Limita-tions in Female Soccer Players Twelve Years after Anterior Cruciate Ligament Injury. Arthritis Rheum. 2004; 50: 3145–3152.
- Piasecki DP, Spindler KP, Warren TA, Andrish, JT, Parker RD, et al. Intraarticular Injuries Associated with Anterior Cruciate Ligament Tear: Findings at Ligament Reconstruction in High School and Recreational Athletes. Am. J. Sports Med. 2003; 31: 601–605.
- Chaudhari AMW, Briant PL, Bevill SL, Koo S, Andriacchi TP. Knee Kinematics, Cartilage Morphology, and Osteo-arthritis after ACL Injury. Med. Sci. Sports Exerc. 2008; 40: 215–222.
- Luc B, Gribble PA, Pietrosimone BG. Osteoarthritis Prevalence Following Anterior Cruciate Ligament Reconstruction: A Systematic Review and Numbers-Needed-to-Treat Analysis. J. Athl. Train. 2014; 49: 806–819.
- Cristiani R, Mikkelsen C, Forssblad M, Engström B, Stålman A. Only one patient out of five achieves symmetrical knee function 6 months after primary anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2019; 27: 3461-3470.
- Kakavas G, Malliaropoulos N, Bikos G, Pruna R, Valle X, et al. Periodization in Anterior Cruciate Ligament Rehabilitation: A Novel Framework. Med Princ Pract. 2021; 30: 101-108.
- Herman DC, Pritchard KA, Cosby NL, Selkow NM. Effect of Strength Training on Jump-Landing Biomechanics in Adolescent Females. Sports Health. 2022; 14: 69-76.
- Yoshimizu R, Nakase J, Okuda M, Asai K, Kimura M, et al. Ligamentization of the recon-structed ACL differs between the intraarticular and intraosseous regions: A quantitative assessment using UTE-T2* mapping. PLoS One. 2022; 17: e0271935.
- Cronström A, Tengman E, Häger CK. Risk Factors for Contra-Lateral Secondary Anterior Cruciate Ligament Injury: A Sys-tematic Review with Meta-Analysis. Sports Med. 2021; 51: 1419-1438.
- Hasani S, Feller JA, Webster KE. Familial Predisposition to Anterior Cruciate Ligament Injury: A Systematic Review with Me-ta-analysis. Sports Med. 2022; 52: 2657-2668.