
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Adventitial cystic disease of the common femoral vein
Kwon Cheol Yoo; Lee Chan Jang*
Department of Surgery, Chungbuk National University Hospital, 776 1 Sunhwan-ro, Seowon-gu, Cheongju 28644, Korea.
*Corresponding Author : Lee Chan Jang
Department of Surgery, Chungbuk National University Hospital, 776 1 sunhwan-ro, Seowon-gu, Cheongju 28644, Korea.
Tel: 82-43-269-6337, Fax: 82-43-266-6037;
Email: lcjang@chungbuk.ac.kr
Received : Jan 08, 2023
Accepted : Jan 25, 2023
Published : Feb 01, 2023
Archived : www.jcimcr.org
Copyright : © Jang LC (2023).
Citation: Yoo KC, Jang LC. Adventitial cystic disease of the common femoral vein. J Clin Images Med Case Rep. 2023; 4(2): 2266.
Introduction
Adventitial Cystic Disease (ACD) is a rare vascular disease which is characterized by the accumulation of mucinous components histologically similar to ganglia in the adventitia of a blood vessel. ACD can compress the lumen of blood vessels extrinsically. With respect to ACD, the arterial system is more frequently involved than venous system. Especially, popliteal and femoral artery were most frequently involved. ACD is often misdiagnosed as deep vein thrombosis (DVT), when it is involved with the venous system. The first case of ACD was reported in 1947, which was described in the external iliac artery [1]. A total of four cases have been reported in Korea until now, including two ACD of femoral veins [2,3] and two ACD of external iliac vein [4,5]. Until 2016, 45 cases of venous ACD had been reported in the English literature [6]. The most common symptom of venous ACD is asymmetric lower extremity swelling worsening over time. We report successfully treated ACD case found in transitional zone between right common femoral and external iliac vein below inguinal ligament.
Case report
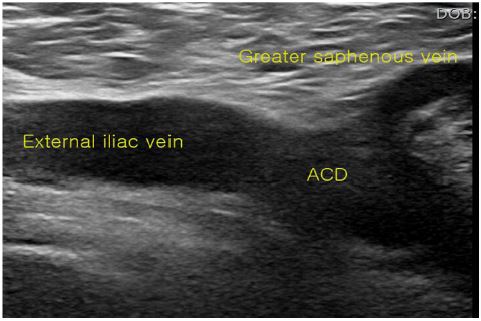
A 60-year-old man presented with right leg edema that had occurred 2 weeks ago. He had no specific past medical history including trauma, operation and intervention. There was no palpable mass at right groin. A circumference of his right mid-thigh was 10 cm longer than left thigh. No other abnormality except right leg swelling was found on physical examination. The level of FDP, d-dimer were normal. An ultrasonography (Figure 1) indicated a segmental occlusion of within the right common femoral and external iliac vein below inguinal ligament. There was no clot in Superficial Femoral Vein (SFV) and proximal iliac vein but SFV was resistant to compression with a probe.
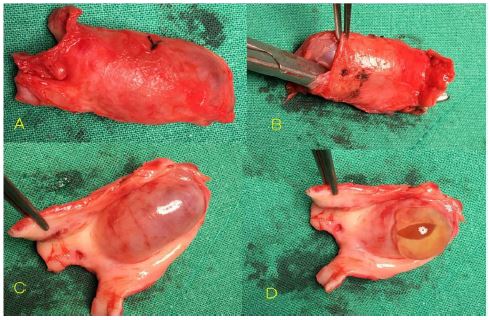
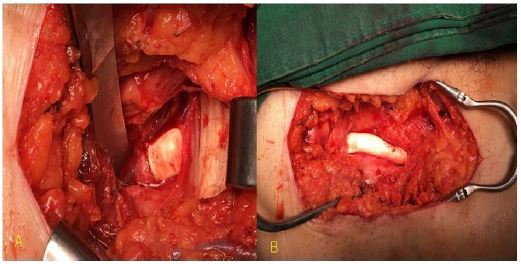
We decided to operate without further studies because deep vein thrombosis was not found. A longitudinal incision was made at right groin. A common femoral and external iliac vein were exposed and isolated. A soft mass was palpable at the vein wall. After proximal and distal control of veins, 4cm vein segment was resected (Figure 2). A protruding inner mass of vein was found. A gelatinous material was coming out from cystic mass. A five centimeter of 10mm PTFE was interposed between veins (Figure 3).
After operation, his leg edema was markedly improved. An anticoagulation was initiated with systemic heparin and switched to warfarin. A postoperative period was uneventful and successful. After 3 months’ anticoagulation, he has been taking aspirin continuously.
Discussion
Adventitial cystic disease is an uncommon condition in venous system. The disease is characterized by a mucin-containing cyst which forms in the wall of the artery or vein, and its etiology is yet unclear. A cystic mass in blood vessel causes symptoms of intermittent claudication in artery [1] and leg swelling in vein. Adventitial cystic disease has also been founded in the external iliac artery, the femoral artery, in branches of the popliteal artery, and the radial, the ulnar arteries in upper extremity. Fewer than 50 cases of adventitial cystic disease of the vein have been introduced in the previous studies [5-7].
The cause of adventitial cystic disease remains uncertain, but there are several theories [4,6,8,9]. Several etiologies, such as ectopic aganglionosis, repeated microtrauma, degeneration of the adventitia due to connective tissue diseases, have all been discussed in the previous reports. The uniloculated or multiloculated cyst was confirmed in pathologist’s report [1,11]. According to the disease progression, an expanding cyst destructs the elastic tissue between the medium and the adventitia of the vein wall that is changed to fibrous connective tissue. Usually, acute or chronic inflammation was not observed. Fibrous connective tissue forms the wall of cyst, and an eosinophilic mucoid gel which is made of mucoproteins and mucopolysaccharides is in cyst.
For the diagnosis of adventitial cystic disease of the vein, the history of patient, further physical examinations and the image findings are needed [12]. Ascending venogram shows the stenosis which has smooth and curvilinear wall with a spiral or hour-glass shape [2,11,13,14]. The significant feature of CT scan was luminal eccentric compression of vein due to a cystic mass which had thin wall with an enhanced rim. No enhancement was observed in the mucinous cyst contents and had intermediate attenuation values between wall and lumen.
A femoral aneurysm, ganglion cyst, lipoma, smooth muscle tumor, sexual tumor and lymphadenopathy should be differentiated.
There are several kinds of treatment methods such as excision after evacuation, vein resection with interposition, aspiration, drainage with sclerosis and fenestration. A recurrence rate of ACD is variable with different treatments. A recurrence rate of cystic aspiration was higher than other methods. We resected a segment of vein with cyst completely and interposed with artificial graft. So far, there is no recurrence.
Conclusion
To sum up, adventitial cystic disease of the vein is a disease that is not frequently reported, but it should be suspected for patients with leg swelling without any risk factors for deep vein thrombosis, with normal FDP and d-dimer, especially when extrinsic mass appears on the diagnostic investigations.
References
- Atkins HJB, Key JA. A case of myxomatous tumour arising in the adventitia of the left external iliac artery. Br J Surg. 1947; 34: 426-427.
- Seo JY, Chung DJ, Kim JH. Adventitial cystic disease of the femoral vein: a case report with the CT venography. Korean J Radiol. 2009; 10: 89-92.
- Cho K, Shin TB. A case of adventitial cystic disease of the femoral vein. J Korean Soc Vasc Surg. 2005; 21: 186-189.
- Cho SH, Shin HW, Lee YG, Koo MJ. Adventitial cystic disease of the left external iliac vein: A case report. J Korean Radiol Soc. 2005; 53: 285-288.
- Kang JM, Choi ST. Adventitial Cystic Disease of the External Iliac Vein in a Patient Presenting with Leg Edema. Korean J Vasc Endovasc Surg. 2009; 25: 163-166.
- Bascone C, Iqbal M, Narh-Martey P, Szuchmacher M, Cicchillo M, et al. Venous Adventitial Cystic Disease: A Review of 45 Cases Treated Since 1963. Int J Vasc Med. 2016; 2: 1-6.
- Velasquez G, Zollikofer C, Nath HP, Barreto A, CastanedaZuniga W, et al. Cystic arterial adventitial degeneration. Radiology. 1980; 134: 19-21
- Dix FP, McDonald M, Obomighie J, Chalmers N, Thompson D,, et al. Cystic adventitial disease of the femoral vein presenting as deep vein thrombosis: a case report and review of the literature. J Vasc Surg. 2006; 44: 871-874.
- Gagnon J, Doyle DL. Adventitial cystic disease of common femoral artery. Ann Vasc Surg. 2007; 21: 84-86.
- Fukui S, Paraskevas N, Lafaurie C, Soury P, Gigou F, et al. Cystic formation compressing the femoral vein: synovial hip joint or adventitial cyst. EJVES Extra. 2004; 8: 1-4.
- Do DD, Braunschweig M, Baumgartner I, Furrer M, Mahler F. Adventitial cystic disease of the popliteal artery: percutaneous US-guided aspiration. Radiology. 1997; 203: 743-746.
- Maldonado-Fernandez N, Lopez-Espada C, Moreno-Escobar J, Martinez-Gamez J, Rodriguez-Morata A, et al. Recurring adventitial cyst in the left external iliac vein. EJVES Extra. 2004; 8: 10-14.
- Wilbur AC, Woelfel GF, Meyer JP, Flanigan DP, Spigos DG. Adventitial cystic disease of the popliteal artery. Radiology. 1985; 155: 63-64.
- Jasinski RW, Masselink BA, Partridge RW, Deckinga BG, Bradford PF. Adventitial cystic disease of the popliteal artery. Radiology. 1987; 163: 153-155.