
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
An unusual complication of ureteric obstruction after transplant Kidney biopsy: A case report
Tarun Kaushik; Munawar Dijoo; Sanjeev Gulati*
Department of Nephrology Flt Lt, Rajan Dhall Fortis Hospital, New Delhi 110070, India.
*Corresponding Author : Sanjeev Gulati
Department of Nephrology Flt Lt. Rajan Dhall Fortis Hospital, Aruna Asaf Ali Road, Vasant Kunjew Delhi 110070, India.
Email: sgulati2002@gmail.com
Received : Jan 11, 2023
Accepted : Jan 25, 2023
Published : Feb 01, 2023
Archived : www.jcimcr.org
Copyright : © Gulati S (2023).
Keywords: Kidney biopsy; Obstruction; Kidney transplant.
Citation: Kaushik T, Dijoo M, Gulati S. An unusual complication of ureteric obstruction after transplant Kidney biopsy: A case report. J Clin Images Med Case Rep. 2023; 4(2): 2267.
Introduction
Percutaneous renal biopsy was an incidental discovery when physicians obtained renal tissue accidentally while performing intended liver biopsies. Subsequently, Iversen and Brun in Copenhagen described their results using cutting and aspiration techniques in 1951 [1]. However, the success was inconsistent and operator-dependent.
Robert M Kark et al. developed the Vim - Silverman biopsy needle and described the kidney biopsy technique in the prone position. The advocacy for this new technique and the training of physicians by the group led to broader acceptance of renal biopsy [2]. The advances in histopathology techniques, including immunofluorescence and electron microscopy, over the last 50 years have made kidney biopsy a cornerstone of nephrology practice.
Percutaneous biopsy of a native or transplant kidney is a routine procedure done under real-time ultrasound guidance by trained personnel. Although rare, bleeding, and associated complications after kidney biopsy may give rise to significant morbidity requiring invasive interventions. Risk stratification from extensive studies has led to further improvement in the safety of kidney biopsies utilizing mitigation of correctable risk factors and better post-biopsy monitoring protocols. We present a rare case of late presentation of kidney transplant uretericobstruction after a kidney biopsy.
Case report
A forty-four year old female patient of Afro-Caribbean origin was noted to have transplant kidney dysfunction. The patient underwent a living related kidney transplant 11 years ago. The cause of CKD was unknown. Her baseline serum creatinine was 1.0, with no significant abnormality on urine analysis. The patient also reported suboptimal immunosuppression compliance due to the poor availability of tacrolimus in her native country.
Investigations revealed – Sodium 138 mmol/l, Potassium 4.0mmol/l, BUN 58 Creatinine 2.2 mg/dl. Hb 10.2 gm/dl TLC 4.6 thou/ul. Platelets 175 thou/l. Prothrombin time 15 seconds. APTT 28 seconds. A urine routine examination showed – Protein-negative, Blood-negative and Pus cells – 20 to 30 per high power field. Urine culture was negative for any growth.
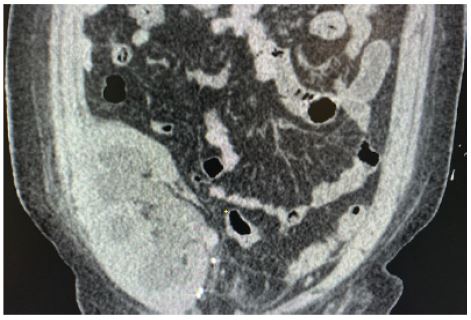
The patient proceeded to have a real-time ultrasound-guided transplant kidney biopsy under local anaesthesia. 18 G spring-loaded automatic biopsy needle was used. Two cores were taken from the upper pole. Blood pressure before the procedure was stable at 110/80 mmHg. An ultrasound scan after the biopsy showed evidence of bleeding in the collecting system (Figure 1). A blood clot of approximately 60 cc in the bladder was also noted. Hematuria with no blood clot was noted. The patient remained hemodynamically stable post-procedure. At 24 hours post-procedure, Urine output was 2800 ml, and hemoglobin was 9.8 gm/dl.
At 48 hours post-biopsy, Mild hematuria persisted with no clots. Haemoglobin was 9.5 gm/dl. A urine culture was sent. The patient had to be discharged due to personal reasons, with a plan for close follow-up.

Subsequently, renal function improved with a creatinine of 3.70 mg/dl on discharge. The kidney biopsy showed severe IFTA stage 3, 80% global glomerulosclerosis and underlying membranous glomerulopathy. At 96 hours, the patient presented with postural symptoms, pain over the kidney transplant graft, low-grade fever, and reduced urine output. The blood pressure on presentation was 60/30 mmHg. Investigations revealed Hb- 8.5 mg/dl, Total leucocyte count 42,000, Serum Creatinine 4.36 mmol/l, BUN 70, Sodium 138, Potassium 4.7, Lactate 3.5, and mild metabolic acidosis with serum bicarbonate of 18 mmol/l. Subsequent urine culture showed multi-drug-resistant pseudomonas species. The patient was admitted to the intensive care unit. The urine output improved after improvement in blood pressure with low-dose ionotropic support. The patient required a total hospital stay of 6 days, including two days in the Intensive care unit. On discharge, the renal function improved with serum Creatinine of 2.1 mmol/lit. Antibiotics were continued for a total of 2 weeks duration. One week after release, the ureteric stent was removed. The repeat urine culture was negative. The patient remained clini-cally stable on outpatient follow-up reviews.
Discussion
In the current era, percutaneous kidney biopsies are done under real time ultrasound guidance using spring-loaded kidney biopsy needles under local anaesthesia. The commonly used automatic spring-loaded kidney biopsy needles are sizes 14-, 16-, or 18-gauge needles (outer diameter of 2.11, 1.65, and 1.27 mm, respectively). The diagnostic yield is typically 10-20 glomeruli with 14 and 16-gauge needles, while 18- gauge needles are associated with slightly lower output in some studies [3]. However, higher gauge needles are associated with higher rates of transfusion when 14 G needles (rate 2.1%) were compared with 18 G needles (0.6%) [4].
In a systematic review of 87 studies, including 118,604 natives and percutaneous kidney biopsies, the approximate incidence of the different bleeding complications was pain at the biopsy site – 4.3 percent, Transient macroscopic haematuria – 3.5 percent, Perinephric hematomas – 11 percent, Erythrocyte transfusion – 1.6 percent IR intervention to control bleeding – 0.3 percent. Nephrectomy to control bleeding – 0.01 percent and Death – 0.06 percent [5].
Most complications were noted to be within the first 6 hours at 77%, while between 6 to 12 hours, 13%, and 7.4% were reported between 12 and 24 hours post kidney biopsy [6].
The risk factors of erythrocyte transfusion following kidney biopsy are systolic blood pressure greater than or equal to 130 mmHg – 1.4 versus 0.1 percent, Serum creatinine greater than or equal to 2 mg/dL (177 micromol/L) – 2.1 versus 0.4 percent, Age over 40 years – 1 versus 0.2 percent and AKI [7]. Haemoglobin concentration less than 12 g/dL has also shown a 2.6 versus 0.5 percent higher risk of post-kidney biopsy bleeding [7].
Post-kidney biopsy ureteric obstruction secondary to blood clots is a rare complication following a kidney biopsy. The timing of these presentations ranged from < 24 h in published cases up to 9 days postbiopsy in native kidney biopsies compared to other biopsy-related complications, which present within 24 hours. Immediate haematuria is usually observed preceding obstructive symptoms. However, intervention such as ureteric stent insertion or percutaneous nephrostomy is required to relieve symptoms.
O’Hara et al. published a case series of 5 cases of post-kidney biopsy ureteric obstruction in 4 Australian hospitals over a period of 4 years. A literature search showed 11 case reports of post-kidney biopsy ureteric obstruction. Of these reported cases, eight patients developed post transplant biopsy ureteric obstruction.
Two patients required transplant ureteric stenting; one patient had percutaneous nephrostomy lasting for three days; one patient had obstruction relieved during nephrostogram; one patient had incidental ureteric stenosis, while the outcome of 3 patients with transplant ureteric obstruction post-kidney biopsy was not reported.
Ureteric obstruction following kidney biopsy is a rare but significant complication. Prior to this case report, only 8 cases have been reported for transplant ureteric obstruction after kidney biopsy [8]. Even at our centre, this is the first case report of ureteric obstruction over more than a decade, with an average number of kidney biopsies of 120 per year. In addition, acute obstruction can give rise to significant morbidity, particularly in transplant kidney biopsy, as the underlying cause for the requirement of kidney biopsy loses focus while managing the iatrogenic complication post-kidney biopsy.
Obstruction should be considered a significant differential diagnosis in patients with prolonged macroscopic haematuria who present with further worsening renal function post-kidney biopsy. The low prevalence of post-biopsy ureteric obstruction could also be due to under-reporting from centres with a high number of kidney biopsies.
References
- Cameron JS, Hicks J. The introduction of renal biopsy into nephrology from 1901 to 1961: A paradigm of the forming of nephrology by technology. Am J Nephrol. 1997; 17: 347–358.
- KARK RM. Renal biopsy. Br Med J. 1955; 1: 535.
- Hogan JJ, Mocanu M, Berns JS. The Native Kidney Biopsy: Update and Evidence for Best Practice. Clinical Journal of the American Society of Nephrology. 2016; 11: 354–362.
- Corapi KM, Chen JLT, Balk EM, Gordon CE. Bleeding Complications of Native Kidney Biopsy: A Systematic Review and Meta-analysis. American Journal of Kidney Diseases. 2012; 60: 62–73.
- Poggio ED, McClelland RL, Blank KN, Hansen S, Bansal S, Bomback AS, et al. Systematic Review and Meta-Analysis of Native Kidney Biopsy Complications. Clinical Journal of the American Society of Nephrolo-gy. 2020; 15: 1595–602.
- Prasad N, Kumar S, Manjunath R, Bhadauria D, Kaul A, Sharma RK, et al. Real-time ultrasound-guided percutaneous renal biopsy with needle guide by nephrologists decreases post-biopsy complications. Clin Kidney J. 2015; 8: 151–156.
- Palsson R, Short SAP, Kibbelaar ZA, Amodu A, Stillman IE, Rennke HG, et al. Bleeding Complications After Percutaneous Native Kidney Biopsy: Results From the Boston Kidney Biopsy Cohort. Kidney Int Rep. 2020; 5: 511–508.
- O’Hara DV, Wong JK, Cooper B, Wong G, Wong MG, Cheikh Hassan HI, et al. Lessons for the clinical nephrologist: Ureteric obstruction secondary to blood clot after kidney biopsy. J Nephrol. 2021; 34: 2131–2136.