
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Lens-induced uveitis following pars plana vitrectomy
Seyedeh Maryam Hosseini; Ghodsieh Zamani; Mohammadreza Rastegar; Javad Sadeghi Allah Abadi; Mehrdad Motamed Shariati*
Eye Research center, Mashhad University of Medical Science, Iran.
*Corresponding Author : Mehrdad Motamed Shariati
Eye Research Center, Khatam Al-Anbia eye hospital, Gharani boulevard, Mashhad, Iran.
Tel: +989377388690;
Email: Mehrdad_shariati2005@yahoo.com.
Received : Jan 12, 2023
Accepted : Jan 27, 2023
Published : Feb 03, 2023
Archived : www.jcimcr.org
Copyright : © Shariati MM (2023).
Abstract
Background: To report an unusual case of severe anterior segment inflammation with nodular iris infiltration 2 weeks after an uncomplicated Pars Plana Vitrectomy (ppvit) masquerading as endophthalmitis.
Case presentation: A 43-year-old man came to the clinic with severe pain, redness, and vision decrement in his right eye two weeks after uncomplicated pars plana vitrectomy with silicone oil tamponde for rhegmatogenous retinal detachment. Ophthalmic examinations of theright eye revealed mild corneal edema and severe granulomatous type of fibrinous and cellular reaction in the aqueous with nodular iris infiltration. Regarding the progressive cortical cataract, the patient was scheduled for phacoemulsification. During the second surgery, we found a ruptured posterior lens capsule with cortical material floating in the silicone oil-filled vitreous cavity.
Conclusions: The diagnosis of lens-induced uveitis secondary to intraoperative lens injury during vitrectomy should be kept in mind in the case of severe post-operative uveitis.
Keywords: Uveitis; Pars plana vitrectomy; IRIS infiltration; Phacogenic uveitis; Lens-induced uveitis; Endophthalmitis; Autoimmune uveitis.
Citation: Hosseini SM, Zamani G, Rastegar M, Abadi JSA, Shariati MM, et al. Lens-induced uveitis following pars plana vitrectomy. J Clin Images Med Case Rep. 2023; 4(2): 2270.
Background
Postoperative inflammation is one of the most well-known complications of ocular surgery, including Pars Plana Vitrectomy (ppvit). Sterile uveitis following ppvit is usually seen immediately after surgery, is mild, and improves with the use of steroidal anti-inflammatory eye drops with minimal side effects [1]. Various factors such as patient age, duration of surgery, history of uveitis, andconcomitant cataract surgery can affect the occurrence of uveitis following ppvit [2]. If severe inflammation is observed after a single ppvit (without any concomitant intraocular surgery like phacoemulsification, glaucoma surgery, implantation of secondary intraocular lens, etc.) causes such as endophthalmitis, sympathetic ophthalmia, and lens-induced uveitis secondary to traumatic crystallin lens damage should also be suspected [3,4].s
In this article, we will introduce a patient who suffered from severe inflammation of the anterior segment and nodular infiltration foci on the iris two weeks after ppvit and was finally reoperated with a diagnosis of uveitis secondary to posterior capsule lens rupture.
Case presentation
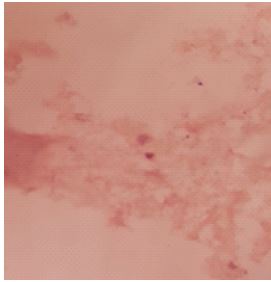
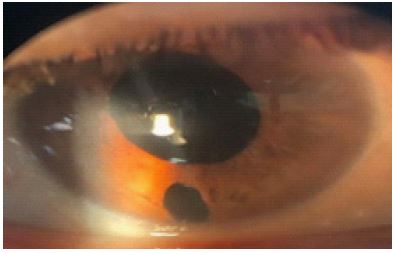
A 43-year-old man came to the clinic because of ocular pain, photophobia, and decreased vision in his right eye since 2 days ago. He underwent ppvit and silicone oil injection as a tampon ding agent due to a nearly total rhegmatogenous retinal detachment two weeks ago. The surgery was done under general anesthesia without significant complications. During the first two weeks after surgery, besides mild corneal edema, the rest of the examinations were unremarkable. The best-corrected visual acuity in the right eye at the time of presentation was counting fingers. Intra Ocular Pressure (IOP) was within normal limits. The anterior segment examination of the right eye showed mild corneal edema, and 4+ aqueous cells and flare (based on SUN Working Group). We found multiple nodular iris infiltrations and posterior synechia. In addition, moderate cortical cataract and fibrin deposition were seen on the anterior lens capsule (Figure 1). Examination of the posterior segment was not possible due to media haziness of severe fibrinous reaction. In ultrasound evaluation, the vitreous cavity was silicone oil-filled and no remarkable pathologic finding was found. The left eye examinations were completely normal. The patient had a history of ppvit and cataract surgery for his left eye three years ago. Regarding the history of previous surgery on the other eye and granulomatous inflammation, we suspected Sympathetic Ophthalmia (SO), however, Indocyanine Green Angiography (ICGA) revealed nothing in the left eye, and during the follow-up, we found no inflammation in the left eye. Due to the exacerbation of inflammation, the patient was treated with a frequent topical steroid (prednisolone 1% eye drop every 2 hours), a topical cycloplegic agent, and systemic corticosteroid (Tab prednisolone 50 mg daily). Initially, the patient partially responded to treatment and his inflammatory symptoms decreased, while after about 2 to 3 weeks, full recovery did not occur. Furthermore, the patient’s crystalline lens opacity increased and progressed to an almost mature cataract during this period. Besides, Intra Ocular Pressure (IOP) decreased to below normal limits (IOP=4 mmHg). Regarding a wax-and-wane type of inflammation, persistent hypotonia, and the impossibility of examining the posterior segment due to media opacity, we scheduled the patient for phacoemulsification. During the second surgery, we found a ruptured posterior capsule with cortical material floating in the silicone oil-filled vitreous cavity and a severe ciliary body infiltration. A sample of the patient’s lens materials was sent to the laboratory for pathological examination. Silicone oil was exchanged and lens material was removed from the vitreous cavity. The patient left aphakic and an inferior peripheral iridectomy was done. Pathology assessment showed few epithelioid cells without atypia and mixed cell infiltration in an acidophilic background (Figure 2). During the postoperative follow-up period, the uveitis completely subsided and the anti-inflammatory drugs were tapered off for 2 months after the surgery, but the eye developed permanent hypotonia (Figure 3).

Discussion
In this report, we introduced a patient with severe anterior segment inflammation 2 weeks after ppvit. Various causes have been expressed for inflammation following an intraocular surgery including Toxic Anterior Segment Syndrome (TASS) and infectious endophthalmitis [5]. These diagnoses specifically TASS, usually occur in the early postoperative period. Furthermore, TASS and infectious endophthalmitis are very rare in the case of ppvit without any concomitant surgery [3,6]. Because ocular inflammation occurred in our patient after two weeks after the surgery, TASS is less relevant in this case. In addition, the presence of silicone oil in the vitreous space, the absence of obvious inflammatory involvement behind the lens-iris diaphragm in the ultrasonography, and the initial response to corticosteroids make the diagnosis of acute postoperative endophthalmitis unlikely.One of the rare but possible diagnoses, in this case, is Sympathetic Ophthalmia (SO) [7]. For this reason, in the initial and follow-up examinations, we looked for the possible presence of inflammation in the other eye. The absence of any evidence of inflammation in the other eye rules out this diagnosis.A notable finding, in this case, is the rapid progression of lens opacity. Cataract with an incidence rate of 12.5% to 80% is one of the most frequent complications following ppvit. Factors such as the patient’s older age, longer duration of surgery, mechanical trauma to the lens during surgery, and the use of gas or silicone oil as tamponading agents at the end of the surgery can all contribute to cataract [8]. If there is no physical contact with the lens during surgery, increased oxygen tension following vitrectomy is one of the main causes of cataracts. Lens opacification in patients following ppvit usually occurs slowly over several months, and its main manifestation is slowly progressive vision loss [9]. The course of cataract progression in our patient indicates the possible mechanism of lens damage during vitrectomy surgery.It seems that in the postoperative period, due to the exposure of the lens proteins, a severe immunological reaction occurred in the anterior segment, and also due to the infiltration of fluid, lens volume increased and cortical cataract progressed. Finally, lens materials are poured into the silicone oil-filled vitreous cavity. While lens damage during ppvit usually occurs in patients with a history of previous ocular trauma or zonular weakness secondary to conditions like pseudoexfoliation [10], our patient had no such risk factors.
Conclusion
It seems that in any case of severe uveitis following ppvit, we should consider the diagnosis of lens-induced uveitis secondary to intraoperative lens injury, even in a case without any risk factor for zonular weakness. In addition, we concluded that phacoantigenic uveitis can be very severe, leading to ciliary shutdown and persistent hypotonia.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials: The datasets used during the current study are available from the corresponding author upon reasonable request.
Competing interests: The authors declare that they have no competing interests.
Funding: The authors received no funding. It is the authors’ work, not funded by the government or academic institutes.
Authors’ contributions: All the authors contributed significantly to this report, and all authors agree to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Acknowledgments: Not applicable.
References
- Halim J, Westcott F, Cascone N, Coombes A. Risk factors associated with postoperative uveitis after cataract surgery: A retrospective case-control study. Eye. 2022; 36: 198-205.
- Romano V, Angi M, Scotti F, Del Grosso R, Romano D,. Inflammation and macular edema after pars plana vitrectomy. Mediators of Inflammation. 2013; 2013.
- Chen G, Tzekov R, Li W, Jiang F, Mao S, et al. Incidence of endophthalmitis after vitrectomy: A Systematic review and meta-analysis. Retina. 2019; 39: 844-852.
- Imen K, Meriam BH, Ilhem S, Sonia A, Nesrine A, et al. Lens-induced hypopyon uveitis as the presenting manifestation of posterior lens nucleus dislocation following pars-plana vitrectomy: Case report. Journal of Ophthalmic Inflammation and Infection. 2021; 11: 1-4.
- Salinger CL, Gaynes BI, Rajpal RK. Innovations in topical ocular corticosteroid therapy for the management of postoperative ocular inflammation and pain. Am. J. Manag. Care. 2019; 25: S215-226.
- Cetinkaya S, Dadaci Z, Aksoy H, Acir NO, Yener HI, Kadioglu E. Toxic Anterior-Segment Syndrome (TASS). Clinical Ophthalmology (Auckland, NZ). 2014; 8: 2065.
- Augsten R, Theis B, Dawczynski J, Voigt U, Königsdörffer E, et al. Sympathetic ophthalmia following pars plana vitrectomy. Klinische Monatsblatter fur Augenheilkunde. 2011; 229: 645.
- Hernandez-Bogantes E, Abdala-Figuerola A, Olivo-Payne A, Quiros F, Wu L. Cataract Following Pars Plana Vitrectomy: A Review. In Seminars in Ophthalmology 2021; 36: 824-831. Taylor & Francis.
- Ji Y, Rong X, Lu Y. Metabolic characterization of human aqueous humor in the cataract progression after pars plana vitrectomy. BMC ophthalmology. 2018; 18: 1-8.
- Kim YC, Lee SJ, Kang KT. Iatrogenic Lens Trauma-induced Glaucoma Following Pars Plana Vitrectomy. Journal of Retina. 2021; 6: 136-138.