
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Spinal acute subdural hematoma following cerebrospinal fluid drainage during thoracoabdominal aortic aneurysm repair: Case report
Duarte Mora Diana Paola1*; Ángel Octavio Donato Rondón2; Luis Orlando Rojas Romero3
1Medical Resident of Neurosurgery, Universidad Militar Nueva Granada, Hospital Militar Central, Transversal 3 No. 49-02, Bogotá, Colombia, Bogotá, Colombia.
2Neuroradiologist, Department of Radiology, Hospital Militar Central, Transversal 3 No. 49-02, Colombia, Bogotá, Colombia.
3Neurosurgeon, Department of Neurosurgery, Hospital Militar Central, Colombia. Transversal 3 No. 49-02, Bogotá, Colombia.
*Corresponding Author : Diana Paola Duarte Mora
Medical Resident of Neurosurgery, Universidad Militar Nueva Granada, Hospital Militar Central, Transversal 3 No. 49-02, Bogotá, Colombia, Bogotá, Colombia.
Email: tdianaduarte05@gmail.com
ORCID: 0000-0003-2035-1994
Received : Dec 07, 2022
Accepted : Jan 30, 2023
Published : Feb 06, 2023
Archived : www.jcimcr.org
Copyright : © Mora DPD (2023).
Abstract
During repair of abdominal aortic aneurysms, the risk of acute spinal cord injury secondary to decreased spinal perfusion rises up to 20%, that`s why the lumbar cerebrospinal fluid drain has been used as a form of intra-spinal pressure control and monitoring medullary perfusion pressure; the positioning of a lumbar drain carries some risks such as cerebrospinal fluid fistula, post-puncture headache or over drainage of cerebrospinal fluid that leads to the development of intracranial subdural hematomas; The case of an acute spinal subdural hematoma is presented after the positioning of a spinal catheter for drainage of cerebrospinal fluid and its surgical management.
Keywords: Spinal subdural hematoma; Lumbar cerebrospinal fluid drainage.
Citation: Paola DMD, Rondón AOD, Romero LOR. Spinal acute subdural hematoma following cerebrospinal fluid drainage during thoracoabdominal aortic aneurysm repair: Case report. J Clin Images Med Case Rep. 2023; 4(2): 2273.
Background and importance
The risk of acute spinal cord injury secondary to decreased perfusion during endovascular repair of thoracic or abdominal aortic aneurysms rises to 20%. For decades, lumbar CSF drainage has been used to decrease intraspinal pressure and improve spinal cord perfusion. However, the lumbar drain placement involves the risks inherent in doing a lumbar puncture. Intracranial subdural hematomas following CSF over drainage from a lumbar drain have been described; however, spinal subdural hematomas develop rarely following a lumbar drain placement.
Clinical Presentation
A 74-year-old woman with a history of arterial hypertension, chronic obstructive pulmonary disease, smoking, and a fusiform thoracoabdominal aortic aneurysm presented with a clinical picture of 8 days of evolution consisting of localized interscapular stabbing pain irradiating into the left hemithorax. The aneurysm extended from the proximal third of the thoracic aorta to the origin of the renal arteries, had an extensive eccentric mural thrombus without signs of dissection or wall bruising, and exerted pressure on the heart. The patient was hospitalized for endovascular repair of the thoracic aortic aneurysm. Before this procedure, a spinal catheter was placed for CSF drainage and monitoring of intrathecal pressure and spinal cord perfusion pressure due to the high risk of spinal cord ischemia. There were some technical difficulties during catheter placement, and multiple punctures were required.
Around 24 hours after the procedure, the patient complained of pain in the right lower limb associated with hypoesthesia; the intrathecal pressure was 30 mmHg. Therefore, analgesia was optimized, and measures to maintain the spinal cord perfusion pressure were adopted. Notwithstanding, the patient’s condition worsened due to lumbar pain and loss of strength in the right lower limb; therefore, the spinal catheter was removed, and computerized tomography (CT) of the thoracic and lumbar spine was performed (Figures 1 and 2). The CT scan showed a subdural hematoma extending from the C4 level to the lumbosacral region with a compressive effect on the medulla and the posterior nerve roots of the cauda equina.

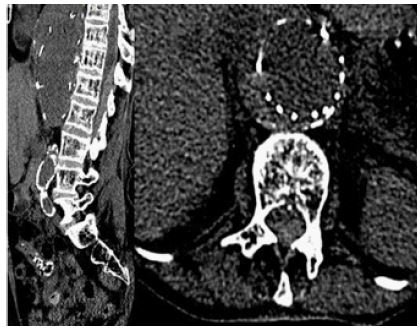
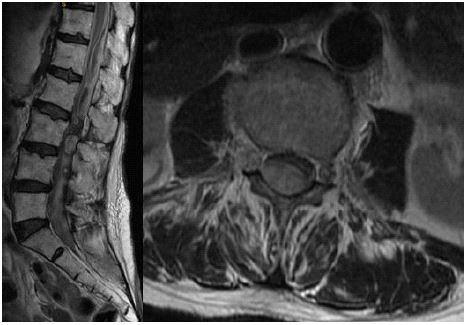
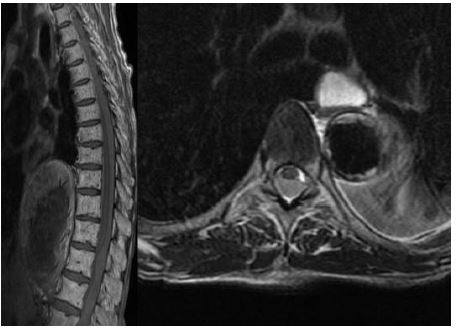

The CT imaging of a subdural hematoma, extending from C4 to the lumbosacral region, was confirmed by Magnetic Resonance Imaging (MRI) of the thoracic and lumbar spine (Figures 3 and 4).
Given the symptoms and findings previously described, a laminectomy at the L3 level was performed to explore the medullary canal. An acute subdural hematoma compressing the nerve roots in the cauda equina was found (Figure 5). The hematoma was drained, and the subdural space was washed in cephalad and caudal directions until clear fluid returns.
In the postoperative period, thrombocytopenia was documented; however, the strength of both lower limbs, predominantly the left one, improved. Additionally, the patient developed neuropathic pain down the right leg that was adequately managed with analgesics.
Discussion
The risk of acute spinal cord injury secondary to hypoperfusion during endovascular repair of thoracic and abdominal aortic aneurysms rises to 20%. For this reason, the use of lumbar CSF drainage is indicated to decrease the intraspinal pressure; this way, the spinal cord perfusion improves, and the risk of spinal cord injury decreases to 2.3% [1]. However, the CSF drainage can associate with some complications; they involve post puncture headache, catheter fracture, meningitis, or the development of intracranial subdural hematomas due to CSF over drainage [2,3].
The incidence of intracranial subdural hematoma secondary to CSF drainage varies from 0.45% to 5.5%, with mortality rates from 11% to 40% due to coagulopathies or CSF fistulas at the puncture site that can be managed with a blood patch [4,5].
Intrathecal hematomas following lumbar puncture are more frequent in the epidural than in the subdural and subarachnoid spaces. Their incidence is around 3%, and their compressive effect on the neural structures require immediate surgical drainage [6,7]. The dura mater is externally composed by elongated fibroblasts and large amounts of collagen, and internally by fibroblasts with few intercellular junctions and extracellular spaces without collagen. The adjacent arachnoid layer is a strong barrier with many intercellular junctions leaving no space between it and the dura mater. For this reason, the space generated by a hematoma, caused by trauma or other pathological problem, is located within the inner dura layer [7,8].
A preexisting bleeding disorder (thrombocytopenia, or therapies with anticoagulants, vitamin K antagonists, and platelet antiaggregants) is a risk factor for developing intrathecal hematomas following a lumbar puncture with a worse neurological outcome within 6 and 12 months [9,10].
There is no particular recommendation about the management of hematomas because the neurological outcome for patients undergoing medical and surgical approaches do not differ significantly. This failing is due to the scarce publications on this topic and the high variability of the parameters analyzed (time of evolution of the symptoms, cause of the hematoma, patient’s refusal of surgery, conditions that make patients poor candidates for surgical intervention) among the patients enrolled in different studies.
Conclusion
We present the case of an acute cervicothoracic lumbar subdural hematoma following the placement of a spinal catheter for CSF draining and intrathecal pressure monitoring during the endovascular repair of a thoracoabdominal aortic aneurysm. The hematoma developed as a consequence of thrombocytopenia and multiple lumbar punctures. It was surgically drained in the area of the greatest neural compression, evidenced by the patient’s clinical condition and the radiological images. The neurological outcome was adequate.
Consent: The patient authorizes the publication of this manuscript
Conflict of Interest: None.
Disclosure of Funding: None