
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 4
Diagnosis and surgical management of two cases of spontaneous heterotopic pregnancy
Daniele Neola1; Maria Teresa Musone1; Raffaele Riccardi1; Ennio Conte1; Massimiliano Pellicano1; Marcello Granata1; Giuseppe Maria Maruotti2; Maurizio Guida1; Laura Sarno1*
1Department of Neurosciences, Reproductive Sciences and Dentistry, University Federico II, Via Pansini 5, 80131, Naples, Italy.
2Department of Public Health University Federico II, Via Pansini 5, 80131, Naples, Italy.
*Corresponding Author : Laura Sarno
Department of Neurosciences, Reproductive Sciences and Dentistry, University Federico II, Via Pansini 5, 80131, Naples, Italy.
Email: laura.sarno@unina.it
Received : Dec 08, 2022
Accepted : Jan 31, 2023
Published : Feb 07, 2023
Archived : www.jcimcr.org
Copyright : © Sarno L (2023).
Abstract
Heterotopic pregnancy (HP) is a rare condition, with an incidence of 1/30,000 after spontaneous conception, which increases to 1/1,000-1/100 following assisted reproduction technology (ART), but potentially life-threatening, since the rupture of EP may lead to major internal bleeding, hemoperitoneum and hypovolemic shock. The early and accurate diagnosis of HP is critical to prevent such complications, but it is difficult to develop a defined diagnostic algorithm, since clinical presentation of HP is varied and about 50% of HP patients can be totally asymptomatic. Experience about HP after spontaneous conception is very limited, consisting mostly of case reports or small case series. Thus, there is still lack of defined recommendations for HP management and a lot is left to clinician’s expertise. The extrauterine pregnancy needs to be terminated using minimally invasive techniques without disturbing the intrauterine gestational sac. We report two cases of HP after spontaneous conception at our center, treated with surgical approach, one laparoscopic and the other one laparotomic since patient had Sars-Cov2 infection, in order to enlarge knowledge about HP and highlight the importance of early identification, since the delay or failure of diagnosis may lead to major complications, potentially mortal.
Keywords: Heterotopic pregnancy; Ectopic pregnancy; Obstetric emergency; Laparoscopy.
Citation: Neola D, Musone MT, Riccardi R, Conte E, Sarno L, et al. Diagnosis and surgical management of two cases of spontaneous heterotopic pregnancy. J Clin Images Med Case Rep. 2023; 4(2): 2274.
Introduction
Heterotopic pregnancy (HP) is defined as the concurrent presence of two or more pregnancies in different sites. It is most often manifested as the simultaneous occurrence of intrauterine pregnancy (IUP) and ectopic pregnancy (EP) [1].
HP is a rare condition, with an incidence of 1/30,000 after spontaneous conception [2], which increases to 1/1,000-1/100 following assisted reproduction technology (ART) [3-5], but potentially life-threatening, since the rupture of EP may lead to major internal bleeding, hemoperitoneum and hypovolemic shock [6].
Thus, the early and accurate diagnosis of HP is critical to prevent such complications, but it is difficult to develop a defined diagnostic algorithm, since clinical presentation of HP is varied (including vaginal bleeding, acute abdominal pain, cold and pale skin, confusion, weakness, oliguria or anuria, weak pulse and increased heart rate) and about 50% HP patients can be totally asymptomatic [1,7-9]. Serum b-hCG levels are not useful in the diagnosis of a HP due to the co-existence of the IUP [6,10]. Transvaginal ultrasound is an effective exam to diagnose a HP, which presents as an IUP co-existed with an inhomogeneous mass separated from the ovary with or without “ring sign” or fetal pole with or without cardiac activity in an extrauterine location [11,12]. Ectopic placental blood flow, commonly referred to as a “ring of fire”, can be seen with color Doppler within the periphery of an adnexal mass. This hypervascularity can be difficult to distinguish and the HP may be confused as an hemorrhagic corpus luteum cyst [11].
Management of HP remains a challenge even in the hands of an expert obstetrician. The extrauterine pregnancy needs to be terminated using minimally invasive techniques without disturbing the intrauterine gestational sac [13]. Treatment modalities include expectant management, surgical management and sonographic guided embryo aspiration with or without embryo-killing drugs [1,8,14-16].
We report two cases of HP after spontaneous conception at our center, treated with surgical approach, one laparoscopic and the other one laparotomic since patient had Sars-Cov2 infection, in order to share our experience and enlarge knowledge about the management of this rare condition.
Written informed consent was obtained from the patients for publication of this case report and any accompanying images.
Case 1
A 29 years-old primigravida at 7 weeks +2 days of gestation who conceived spontaneously referred to the obstetric emergency service of our hospital reporting acute abdominal pain and vaginal bleeding. She did not report any chronic preexisting condition or previous surgeries.
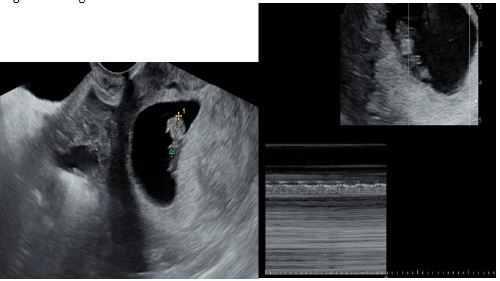
We quickly performed a transvaginal ultrasound, which demonstrated the presence of an intrauterine pregnancy with a crown-rump length of 12 mm, corresponding to the gestational age calculated by last menstrual period, and cardiac activity. In the pouch of Douglas, a mass of 82 x 38 mm in size, with inhomogeneous echogenicity and hematic content and no vascularization at color-Doppler was observed (Figure 1). Both left and right ovaries were normally visualized, and presence of free pelvic fluid (about 20 mm in size) was reported. We hypothesized that the mass was a hematocele due to a ruptured tubal HP. Due to the worsening of symptomatology, we informed the patient of the potential risks of her condition and we decided to perform an urgent laporoscopic exploration. Patient underwent laparoscopic exploration with low-pressure (10 mmHg) pneumoperitoneum, which detected hemoperitoneum due to a ruptured left tubal pregnancy (Figure 2 and Figure 3). In order to preserve intrauterine pregnancy, we performed a laparoscopic left salpingectomy at low pneumoperitoneum pressure with no manipulation of the uterus, associated with hemoperitoneum aspiration and multiple peritoneal washings. Cardiac activity of IUP was checked before, during and after the procedure. Postoperative course was uneventful. Therapy included hydration, antibiotics (1st generation cephalosporins) and intramuscular progesterone. A transvaginal ultrasound was performed 24h and 48 h after the procedure: cardiac activity of IUP was present in both examinations and no free pelvic fluid was detected. The patient was discharged on the second day after surgery. The histological examination of left tube confirmed the HP. The rest of pregnancy was uneventful, and patient delivered spontaneously at 40 weeks without any fetal or maternal complication.
Case 2
A 35 years old gravida III (para II) at 12 weeks +2 days of gestation with a monochorionic diamniotic twin pregnancy, who conceived spontaneously, with Sars-Cov2 infection, was transferred to the Covid-19 obstetrics department of our Centre from another hospital, in which she was diagnosed with hemoperitoneum. Patient attended the Emergency Department of a local hospital due to a lipothymic episode and acute pelvic pain. She had a diagnosis of hemoperitoneum and she was transferred to the COVID Unit of the University Hospital of Naples Federico II, due to the presence of a COVID-19 positive rynopharingeal swab. In her past medical history, she referred only an inguinal hernioplasty performed at the age of 7 and a history of hypothyroidism. On physical examination, the patient appeared in stable condition, with normal vital parameters and the presence of an untreatable abdomen, painful at palpation in all quadrants. An ultrasound scan was performed, showing the presence of monochorionic diamniotic twin pregnancy in the uterus (Figure 4) with cardiac activity present for both fetuses, the presence of fluid in the abdomen that reached the subsplenic and subhepatic recesses. In the right adnexal area, an anechoic area was visualized, which was surrounded by a hyperechoic layer with a vascular ring, compatible with the diagnosis of ectopic pregnancy and rupture of right tube (Figure 4). The patient was informed of her condition and associated risks, and we decided to proceed with an urgent sub-umbilicus-pubic laparotomy, since a laparoscopic operatory room was not available in our Covid-19 obstetrics department. Surgical exploration of the abdomen demonstrated an extensive hemoperitoneum with clots, and approximately 1500 ml of blood were aspirated. At the level of the right adnex, there was a 3 x 3 cm neoformation referable to an EP. The right tube was then removed. In addition, we performed multiple peritoneal washes and applied an intracavitary drainage. Cardiac activity of IUP was checked before, during and after the procedure. In the postoperative period, patient received a blood transfusion due to the lowering of hemoglobin values under 7 g/dl. Therapy included hydration, antibiotics (1st generation cephalosporins), subcutaneous anticoagulant and intramuscular progesterone. A transvaginal ultrasound was performed 24 h and 48 h after the procedure: cardiac activity of IUP was present in both examinations for both fetuses. Patient was discharged on the sixth day after surgery. The histological examination of left tubal confirmed the EP. She is actually at 20 weeks of gestation and pregnancy has been uneventful so far.



Discussion
HP is a rare condition. Spontaneous incidence is 1/30,000 [2], increasing with the presence of risk factors, such as a history of pelvic inflammatory disease (PID) [2] or ovarian stimulation therapy [5,17-19], and rising to approximately 1 in 100 ART pregnancies [20], since the embryos that are placed in the endometrial cavity during ART procedures may not implant immediately onto the endometrium, drifting towards the tubes and predisposing to a HP [13]. Experience about HP after spontaneous conception is very limited, consisting mostly of case reports or small case series [6]. Thus, there is still lack of defined recommendations for HP management and a lot is left to clinician’s expertise.
We reported our experience in order to enlarge knowledge about HP and highlight the importance of early identification, since the delay or failure of diagnosis may lead to major complications, potentially mortal. In fact, the percentage of serious clinical presentations (hemoperitoneum, tubal rupture, acute abdominal syndrome) was demonstrated higher in “spontaneous HP cases” [1,21], probably due to a low HP suspicion in non-ART pregnancies, and most spontaneous HPs are diagnosed after rupture of the EP [22,23].
In case 2, we observed an HP in a patient with monochorionic-diamniotic twin intrauterine pregnancy and after a spontaneous conception. Even if some authors reported an HP triplet with intrauterine twin pregnancies after in vitro fertilization [24], HP spontaneous triplet is a rare event. Kotlyar et al. [25] described a case of HP in a patient with monochorionic monoamniotic intrauterine pregnancy after spontaneous conception. In this case, the diagnosis was made later, in the second trimester, due to the onset of abdominal pain for several days and missed until the onset of complication.
Therefore, these cases outline that a clinical suspicion of HP must not be underestimated in spontaneously conceived pregnancies, even in case of twin pregnancies, although most cases are related with ART. Even if the reported incidence of adnexal mass in early pregnancy is low [26], our cases raise some questions about the importance to check for adnexa in early pregnancy, in order to early identify pathological conditions.
Our report also points up the importance of surgical approach for HP management, which resulted critical for both diagnosis and treatment. In fact, it was demonstrated that ultrasonography makes a definitive diagnosis of HP in about a third of patients [1] only, with surgical exploration being the gold standard. In this regard, laparoscopy was shown to be safe during pregnancy [27] and better than laparotomy in terms of post-surgical recovery [28].
The aim of HP treatment is to remove the EP preserving the IUP, which makes it difficult and challenging [29]. Several approaches were described in literature, with surgical management, especially laparoscopic, being the most indicated in case of hemodynamic instability or ruptured EP [14]. Surgical removal of the EP includes salpingectomy, salpingostomy, cornual resection, oophorectomy and even total abdominal hysterectomy [14]. Conservative treatment to preserve future fertility was widely debated, but it was demonstrated that, particularly in patients with an intact contralateral tube, fertility results after salpingectomy are comparable to those observed after salpingotomy [30,31]. Moreover, radical treatment is easier, thus reducing the risk of complications observed at salpingotomy [1].
Other approaches for HP include expectant management, mostly used in asymptomatic patients [15,32], and transabdominal sonographic guided aspiration of ectopic gestational embryo with or without embryo-killing drug [33,34] (such as potassium chloride and hyperosmolar glucose), which is possible only if the ectopic gestational sac can be clearly identified.
However, due to the lack of randomized controlled trials, it is difficult to establish a standard treatment for HP, therefore a patient-tailored approach should be discussed case by case.
Conclusion
HP is a rare but potentially life-threatening condition, which must be suspected even in absence of risk factors. This case report highlights the importance of early diagnosis, critical to prevent major complications, and the safety and feasibility of surgical approach, which allowed to remove the EP preserving the IUP and so maternal desire of pregnancy. Examination of the adnexa in early pregnancy might improve early diagnosis of pathological conditions and reduce the risk of severe complications.
Conflict of interest statement: Authors report no conflict of interest.
References
- Barrenetxea G, Barinaga-Rementeria L, Lopez de Larruzea A, et al. Heterotopic pregnancy: two cases and a comparative review. Fertil Steril. 2007; 87(2): 417.e9-417.e15. doi:10.1016/j.fertnstert.2006.05.085
- Reece EA, Petrie RH, Sirmans MF, et al. Combined intrauterine and extrauterine gestations: A review. Am J Obstet Gynecol. 1983; 146(3). doi:10.1016/0002-9378(83)90755-X
- Perkins KM, Boulet SL, Kissin DM, et al. Risk of ectopic pregnancy associated with assisted reproductive technology in the United States. 2001-2011. Obstet Gynecol. 2015; 125(1). doi:10.1097/AOG.0000000000000584
- Clayton HB, Schieve LA, Peterson HB, et al. A comparison of heterotopic and intrauterine-only pregnancy outcomes after assisted reproductive technologies in the United States from 1999 to 2002. Fertil Steril. 2007; 87(2).
- Cirillo D, Sardo ADS, Cirillo P, et al. Conservative laparoscopic treatment of heterotopic ovarian and intrauterine pregnancy following ovulation induction with gonadotropins. Acta Obstet Gynecol Scand. 2006; 85(10). doi:10.1080/00016340600613550
- Li JB, Kong LZ, Yang JB, et al. Management of heterotopic pregnancy experience from 1 tertiary medical center. Med (United States). 2016; 95(5): 1-7. doi:10.1097/MD.0000000000002570
- Talbot K, Simpson R, Price N, et al. Heterotopic pregnancy. J Obstet Gynaecol (Lahore). 2011; 31(1): 7-12. doi:10.3109/01443615.2010.522749
- Yu Y, Xu W, Xie Z, et al. Management and outcome of 25 heterotopic pregnancies in Zhejiang, China. Eur J Obstet Gynecol Reprod Biol. 2014; 180(1). doi:10.1016/j.ejogrb.2014.04.046
- Sun SY, Araujo Júnior E, Elito Júnior J, et al. Diagnosis of Heterotopic Pregnancy Using Ultrasound and Magnetic Resonance Imaging in the First Trimester of Pregnancy: A Case Report. Case Rep Radiol. 2012; 2012. doi:10.1155/2012/317592
- Johnson N, McComb P, Gudex G. Heterotopic pregnancy complicating in vitro fertilization. Aust New Zeal J Obstet Gynaecol. 1998; 38(2). doi:10.1111/j.1479-828X.1998.tb02989.x
- Li XH, Ouyang Y, Lu GX. Value of transvaginal sonography in diagnosing heterotopic pregnancy after in-vitro fertilization with embryo transfer. Ultrasound Obstet Gynecol. 2013 ;41(5). doi:10.1002/uog.12341
- Baron KT, Babagbemi KT, Arleo EK, et al. Emergent complications of assisted reproduction: Expecting the unexpected. Radiographics. 2013; 33(1). doi:10.1148/rg.331125011
- Deka D, Bahadur A, Singh A, et al. Successful management of heterotopic pregnancy after fetal reduction using potassium chloride and methotrexate. J Hum Reprod Sci. 2012; 5(1): 57-60. doi:10.4103/0974-1208.97807
- Eom JM, Choi JS, Ko JH, et al. Surgical and obstetric outcomes of laparoscopic management for women with heterotopic pregnancy. J Obstet Gynaecol Res. 2013; 39(12): 1580-1586. doi:10.1111/jog.12106
- Baxi A, Kaushal M, Karmalkar HK, et al. Successful expectant management of tubal heterotopic pregnancy. J Hum Reprod Sci. 2010; 3(2). doi:10.4103/0974-1208.69333
- Ocal P, Erkan S, Cepni I, et al. Transvaginal ultrasound-guided aspiration and instillation of hyperosmolar glucose for treatment of unruptured tubal heterotopic pregnancy. Arch Gynecol Obstet. 2007; 276(3). doi:10.1007/s00404-007-0343-3
- Bello G V., Schonholz D, Moshirpur J, et al. Combined pregnancy: The mount sinai experience. Obstet Gynecol Surv. 1986; 41(10). doi:10.1097/00006254-198610000-00001
- Maruotti GM, Sarno L, Morlando M, et al. Heterotopic pregnancy: It is really a rare event? the importance to exclude it not only after in vitro fertilization but also in case of spontaneous conception. Fertil Steril. 2010; 94(3). doi:10.1016/j.fertnstert.2010.05.001
- Zullo F, Pellicano M, Di Carlo C, et al. Heterotopic pregnancy in a woman without previous ovarian hyperstimulation: Ultrasound diagnosis and management. Eur J Obstet Gynecol Reprod Biol. 1996; 66(2). doi:10.1016/0301-2115(96)02404-9
- Molloy D, Deambrosis W, Keeping D, et al. Multiple-sited (heterotopic) pregnancy after in vitro fertilization and gamete intrafallopian transfer. Fertil Steril. 1990; 53(6). doi:10.1016/s0015-0282(16)53587-0
- Josephy D, Ovadia M, Schonman R, et al. 2278 Spontaneous vs. Assisted Reproductive Technology-related Ectopic Pregnancy – Are There Any Differences? J Minim Invasive Gynecol. 2019; 26(7). doi:10.1016/j.jmig.2019.09.423
- Sayin NC, Yardim T. Live birth of healthy twins after a heterotopic tubal and intrauterine twin pregnancy in a woman who was stimulated with clomiphene citrate. Fertil Steril. 2003; 80(5). doi:10.1016/S0015-0282(03)02168-X
- Fernan dez H, Gervaise A. Ectopic pregnancies after infertility treatment: Modern diagnosis and therapeutic strategy. Hum Reprod Update. 2004; 10(6). doi:10.1093/humupd/dmh043
- Nikolaou DS, Lavery S, Bevan R, et al. Triplet heterotopic pregnancy with an intrauterine monochorionic diamniotic twin pregnancy and an interstitial pregnancy following in vitro fertilisation and transfer of two embryos. J Obstet Gynaecol (Lahore). 2002; 22(1). doi:10.1080/01443610211123
- Kotlyar A, Eaton J, Singh K, et al. Spontaneous heterotopic triplet pregnancy with intrauterine monochorionic-monoamnionic twins. Case Reports Perinat Med. 2016; 5(2). doi:10.1515/crpm-2016-0019
- Condous G, Khalid A, Okaro E, et al. Should we be examining the ovaries in pregnancy? Prevalence and natural history of adnexal pathology detected at first-trimester sonography. Ultrasound Obstet Gynecol. 2004; 24(1). doi:10.1002/uog.1083
- Zheng M, Li X, Ouyang Y, et al. Analysis of the pregnancy outcomes of heterotopic fallopian tubal pregnancy and heterotopic interstitial pregnancy after in vitro fertilization - embryo transfer. Fertil Steril. 2019; 112(3). doi:10.1016/j.fertnstert.2019.07.1169
- Murphy AA, Nager CW, Wujek JJ, et al. Operative laparoscopy versus laparotomy for the management of ectopic pregnancy: a prospective trial**Presented at the 46th Annual Meeting of The American Fertility Society, Washington, D.C., October 13 to 18, 1990. Fertil Steril. 1992; 57(6). doi:10.1016/s0015-0282(16)55070-5
- Buca DIP, Murgano D, Impicciatore G, et al. Early diagnosis of heterotopic triplet pregnancy with an intrauterine and bilateral tubal pregnancy after IVF: A case report. J Obstet Gynaecol (Lahore). 2015; 35(7). doi:10.3109/01443615.2014.993940
- Louis-Sylvestre C, Morice P, Chapron C, et al. The role of laparoscopy in the diagnosis and management of heterotopic pregnancies. Hum Reprod. 1997; 12(5). doi:10.1093/humrep/12.5.1100
- Clausen I. Conservative versus radical surgery for tubal pregnancy: A review. Acta Obstet Gynecol Scand. 1996;75(1). doi:10.3109/00016349609033276
- Sentilhes L, Bouet PE, Gromez A, et al. Successful expectant management for a cornual heterotopic pregnancy. Fertil Steril. 2009; 91(3). doi:10.1016/j.fertnstert.2008.09.072
- Wang M, Chen B, Wang J, et al. Nonsurgical Management of Live Tubal Ectopic Pregnancy by Ultrasound-Guided Local Injection and Systemic Methotrexate. J Minim Invasive Gynecol. 2014; 21(4). doi:10.1016/j.jmig.2014.01.009
- Goldstein JS, Ratts VS, Philpott T, et al. Risk of surgery after use of potassium chloride for treatment of tubal heterotopic pregnancy. Obstet Gynecol. 2006; 107(2 II). doi:10.1097/01.AOG.0000175145.23512.5e