
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Perilunate dislocation in adult male with Larsen’s syndrome: A case report
Ahmad Almigdad*; Ayman Mustafa; Ahmad Alzoubi; Ghandi Almanasir; Motaz Al-Qasaimeh; Hassan Alzoubi
Department of Orthopedic, Royal Medical Services, Amman, Jordan.
*Corresponding Author : Ahmad Almigdad
Department of Orthopedic, Royal Medical Services, Amman, Jordan.
Email: akmigdad_just@yahoo.com
Received : Jan 13, 2023
Accepted : Feb 01, 2023
Published : Feb 08, 2023
Archived : www.jcimcr.org
Copyright : © Almigdad A (2023).
Abstract
Larsen syndrome is a rare genetic disorder of osteochondrodysplasia manifested by distinctive facial features, multiple joint dislocations, and spinal abnormalities. Joint dislocations described in Larsen syndrome include the hip, knee, shoulder and elbow. However, atypical dislocations such as perilunate may also occur in Larsen syndrome.
In this report, we present a 28-year-old adult male who presented with a nontraumatic perilunate dislocation.
Keywords: Larsen syndrome; Perilunate dislocation; Osteochondrodysplasia.
Citation: Almigdad A, Mustafa A, Alzoubi A, Almanasir G, Al-Qasaimeh M, et al. Perilunate dislocation in adult male with Larsen’s syndrome: A case report. J Clin Images Med Case Rep. 2023; 4(2): 2276.
Introduction
Larsen Syndrome (LS) is a rare genetic disorder of osteochondrodysplasia and was first described by Larsen in 1950 [1]. LS is genetically heterogeneous and consists of an autosomal dominant disorder; however, autosomal recessive and sporadic disorders have also been reported [2-4]. Genetic testing is helpful in diagnosing LS patients with atypical or milder clinical manifestations [5]. LS manifests clinically by distinctive facial features, multiple joint dislocations of the hip, knee, and elbow joints, and spinal abnormalities, including scoliosis and cervical kyphosis. Other musculoskeletal manifestations include equinovarus or equinovalgus foot deformities and cylindrically shaped fingers [6-8]. Characteristic craniofacial anomalies include frontal protrusion, depressed nasal bridge, midface hypoplasia, and ocular hypertelorism [9]. Other features, such as cleft palate, occur in 23-50% of patients from LS, and hearing loss results from malformations of the ossicles [10,11].
In this report, we present an adult male who was diagnosed with LS and had been experiencing nontraumatic wrist pain for six months, which we diagnosed as perilunate dislocation. However, we could not determine whether it was a congenital or spontaneous dislocation because the symptoms appeared late and the radiograph of the wrist showed mild arthritic changes.
Case presentation
A 28-year-old male farm worker, who had previously been diagnosed with LS, was referred to the hand clinic at the Royal Rehabilitation Center at King Hussein Medical City in Amman, the capital of Jordan, with a six-month history of left wrist pain. The patient did not recoil any trauma and was initially treated with a splint. He was diagnosed with LS based on clinical findings. At birth, he had a cleft palate and classical craniofacial malformation, including a flat face, prominent forehead, depressed nasal bridge, malar flattening, and ocular hypertelorism. He was admitted to the neonatal intensive care unit due to respiratory distress and stridor, and was found to have subglottic stenosis. The patient underwent tracheostomy and cleft palate surgery at 1.5 years of age. He has laryngomalacia and tracheomalacia, and his stature is short. However, no joint dislocations or spinal problems were noted, and he had no hearing loss. The patient was admitted repeatedly for a recurrent chest infection.
The wrist pain started insidiously and was associated with limited range of motion and mild swelling. The patient neglected the symptoms for months. He then visited a local orthopedic surgeon and the patient’s radiographs showed a perilunate dislocation (Figure 1). Therefore, a removable splint was applied and he was referred to a hand clinic.
The radiograph of the wrist showed that the lunate was subluxated and rotated in the lunate fossa, and the perilunate bones were dislocated. The contralateral right side had hypoplastic carpal bones, especially the trapezoid, trapezium, and scaphoid. An examination of the wrist CT showed cystic changes of the carpal bone with arthritic changes, Figure 2.
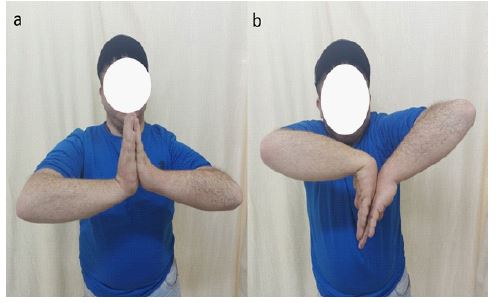
The patient described tolerable pain that increased with activity. Examination revealed mild wrist swelling and tenderness on deep palpation of the wrist, and no neurologic symptoms or deficits were noted. The range of motion of the affected wrist was as follows: Flexion 70°, extension 60°, radial deviation 20°, and ulnar deviation 30° compared with the contralateral wrist (90° flexion and extension, 40° radial and ulnar deviations, Figure 3. The power grip of the left hand was 14 kg compared with 28 kg for the normal right hand. The pinch grip was 7.75 kg on the left side and 8.5 kg on the right side.


The patient reported that his symptoms were relieved with a splint and analgesics. He was counseled about the future consequences of his condition and the possible need for total wrist arthrodesis or radioscapholunate fusion once his pain worsened. The patient was satisfied with the conservative treatment and further management will be based on the evolution of his symptoms.
Discussion
Joint dislocations associated with LS usually involve the large joints, including the hip, knee, shoulder, and elbow, in the form of radial head dislocation. However, joint hypermobility predisposes to multiple joint dislocations [7]. Spinal deformities associated with LS have been extensively described in the literature, with kyphosis of the cervical spine being the most serious orthopedic manifestation and carrying the risk of life-threatening paralysis. Nevertheless, early surgical stabilization of the cervical spine and major joint dislocations play an important role in the treatment of this syndrome [12]. However, to our knowledge, no cases of perilunate dislocation have been reported in the literature as a manifestation of LS.
In this case, we report a 28-year-old adult male who presented with perilunate dislocation in the absence of trauma. However, we cannot determine whether the dislocation was congenital or acquired because wrist radiographs were not available before the onset of symptoms. The patient’s symptoms have been present for six months and he denied any previous symptoms. If we assume that it is a congenital dislocation, we would expect a more destroyed joint on the radiograph in such a chronic dislocation. However, a congenital dislocation is better tolerated by patients than a traumatic dislocation, and the appearance of symptoms could represent the development of arthritic wrist changes in a long-term dislocation. Another suggestion is that it was a recent dislocation because symptoms lasted only a short time and radiographs showed mild changes. However, due to the lack of previous radiographs, we cannot confirm any theory.
Lunate and perilunate dislocations are high-energy wrist injuries and are associated with poor functional outcomes. However, the absence of previous trauma suggests that this dislocation was part of LS. Therefore, we recommend radiographic examination of all joints as soon as LS is suspected.
Conclusion
LS exhibit typical musculoskeletal deformities. Joint dislocations described with LS include the hip, knee, shoulder, and elbow. However, atypical dislocations such as perilunate may also occur in LS. Therefore, asymptomatic joints should also be examined.
References
- Larsen LJ, Schottstaedt ER, Bost FC. Multiple congenital dislocations associated with characteristic facial abnormality. J Pediatr. 1950; 37: 574–581.
- Krakow D, Robertson SP, King LM, Morgan T, Sebald ET, et al. Mutations inthe gene encoding filamin B disrupt vertebral segmentation, joint formation and skeletogenesis. Nat Genet. 2004; 36: 405–410.
- Bicknell LS, Farrington-Rock C, Shafeghati Y, Rump P, Alanay Y, et al. A molecular and clinical study of Larsen syndrome caused by mutations in FLNB. J Med Genet. 2007; 44: 89–98.
- Girisha KM, Bidchol AM, Graul-Neumann L, Gupta A, Hehr U, Lessel D, etal. Phenotype and genotype in patients with Larsen syndrome: Clinicalhomogeneity and allelic heterogeneity in seven patients. BMC Med Genet. 2016; 17: 27.
- Kodra N, Diamonstein C, Hauser NS. A case study of atypical Larsen syndrome with absent hallmark joint dislocations. Mol Genet Genomic Med. 2019; 7: e648.
- Robertson FW, Kozlowski K, Middleton RW. Larsen’s syndrome; Clin Pediatr (Phila). 1975; 14: 53-60.
- Laville JM, Lakermance P, Limouzy F. Larsen’s syndrome: Review of the literature and analysis of thirty-eight cases. J Pediatr Orthop. 1994; 14: 63–73.
- M. Madera, A. Crawford, F.T. Mangano, Management of severe cervical kyphosis in a patient with Larsen syndrome: Case report, J. Neurosurg. Pediatr. 2008; 1: 320–324./li>
- Larsen syndrome. In: Raoul CM, Ian DK, Judith EA, editors. Gorlin’s syndromes of the head and neck. 5rd ed. New York: Academic; 2010; 984–988.
- Stanley CS, Thelin JW, Miles JH. Mixed hearing loss in Larsen syndrome. Clin Genet. 1988; 33: 395–398.
- Marques LHS, Martins DV, Juares GL, Lorenzetti FTM, Monsanto RDC, et al. Otologic manifestations of Larsen syndrome. Int J Pediatr Otorhinolaryngol. 2017; 101: 223–229.
- H Sakaura, T Matsuoka, M Iwasaki, K Yonenobu, H Yoshikawa, et al. Surgical treatment of cervical kyphosis in Larsen syndrome: Report of 3 cases and review of the literature. Spine. 2007; 32: 39–44.