
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Imaging features of Killian polyp in the maxillary sinus: Case report and review of the literature
I Zakariaa*; I Mahdar; M Banao; Pr Laoudiyi; Pr Chbani; Pr Salam
Radiology Pediatric Department, Univeristy Hospital Ibnu Rochd, Casablanca, Morocco.
*Corresponding Author : Ilias Zakariaa
Radiology pediatric department, Univeristy Hospital Ibnu Rochd, Casablanca, Morocco.
Email: zakariailias@gmail.com
Received : Jan 11, 2023
Accepted : Feb 01, 2023
Published : Feb 08, 2023
Archived : www.jcimcr.org
Copyright : © Zakariaa I (2023).
Abstract
The Killian polyp or antrochoanal polyp, represents 4% to 6% of nasal polyps and is more common in children and young adults. This benign lesion grows from the mucosa of the maxillary sinus and extends to the choana. A 7 year-old patient consulted for increasing nasal obstruction. Computed tomography demonstrated a well-defined, hypodense mass in the left maxillary sinus extending to nasopharynx and oropharynx. An excisional biopsy was performed, and histopathology confirmed the diagnosis of a Killian polyp.
Keywords: Antrochoanal polyp; Killian polyp; CT scan.
Citation: Zakariaa I, Mahdar I, Banao M, Laoudiyi Pr, Chbani Pr. Imaging features of killian polyp in the maxillary sinus: Case report and review of the literature. J Clin Images Med Case Rep. 2023; 4(2): 2277.
Introduction
The Killian polyp also known as antrochoanal polyp is a benign polypoid lesion, usually arising from the maxillary sinus. It represents 4% to 6% of all nasal polyps in adults and upto 42% in children [1]. This polypoid lesion represents mucosal growth due to chronic inflammation. In adults, they are generally related to chronic sinusitis, whereas in children allergic polyps are more frequent. However, the risk factors remain unclear. The Killian polyp usually originates in the maxillary sinus and symptoms include nasal obstruction, discharge and dyspnea [1,2]. The polyp can be diagnosed on CT scan. The radiological features are very important to discuss given their undeniable contribution in the diagnosis. Treatment involves surgery and the rate of recurrence depends on the surgical approach.
Case report
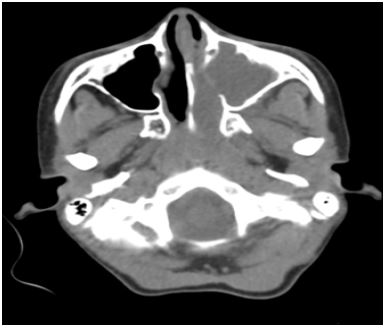
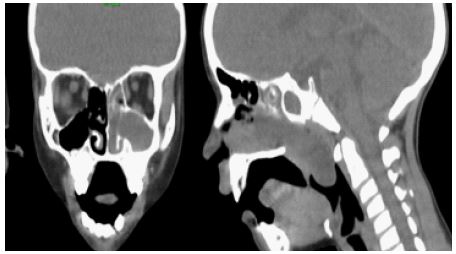
A 7-year-old boy presented to the pediatric emergency department with a history of snoring, sleep apnea and sore throat. No other relevant medical history was noted. CT-scan revealed a soft tissue masse, measuring 70 x 27 x 40 mm, arising from the left maxillary sinus passing through the maxillary ostium and enlarging it, extending to the corresponding nasal cavities and posteriorly into the nasopharynx and oropharynx (Figure 1 and 2). This mass didn’t show enhancement after administration of contrast. There was no erosion or destruction of adjacent bony structures. We also note complete opacification of the homolateral compartment of the sphenoid sinus and the ethmoid air cells. Rhinoscopy and nasofibroscopy revealed a pale polypoidal mass in the left nasal cavity, extending to the nasopharynx. The patient underwent surgery by nasal endoscopy and the mass was removed under general anesthesia. Histopathology confirmed the diagnosis and the patient experience complete recovery with resolution of prior symptoms.
Discussion
The Killian polyp is an inflammatory nasal polyp more frequent in the pediatric population. It was first described as a solitary mass with cystic and solid components in the maxillary sinus and extending to the nasopharynx. Symptoms include nasal obstruction and discharge, epistaxis, snoring and obstructive sleep apnea. The main etiology is still unknown, however research suggests that anatomic abnormalities such as nasal septal deviation, concha bullosa, inferior turbinate hypertrophy, can be a risk factors [2]. The antrochoanal polyp is a benign mucosal growth indicative of chronic inflammation. In adults it is mostly related to chronic sinusitis whereas in children allergic polyps are more common [2,3]. The diagnosis can be challenging, especially in young children (ages from 5 to 8). In this age group there is a wide range of differential diagnoses with resembling symptoms (adenoid hypertrophy, foreign body, malignant tumors…) [4]. A detailed history along with physical examination will help orientate the diagnosis. However, CT-scan and nasal endoscopy represent the gold standard in the diagnosis. Pre-operatively patients must have a sinonasal CT scan, as it provides important information for the surgical intervention [5]. In CT scan images, the antrochoanal polyp usually appears as a hypodense unilateral soft tissue masse occupying the maxillary sinus, extending through the maxillary ostium into the nasal cavity with progression towards the nasopharynx. Widening of the accessory maxillary ostium might be seen due to enlarging cystic portion of polyp. Bony changes (erosion, destruction or sclerosis) are not typically found, if present they are suggestive of a malignant pathology [6]. The patient presented in our case had a similar aspect. Lee suggested a radiological classification based on the appearance of the lesion on CT-scan [7]:
Stage 1: Antronasal polyp without extension to the nasopharynx
Stage 2: Full occlusion of the maxillary sinus ostium with extension to the nasopharynx
Stage 3: Partial occlusion of the maxillary sinus with extension to the nasopharynx
MRI may be used due to the lack of radiation exposure, especially in children. It shows hypointense signal in T1 weighted images, hyperintense in T2 weighted images with peripheral enhancement of the cystic part after administration of gadolinium. In cases with protein content, we may find areas of increased signal on T1 weighted images and intermediate signal on T2 weighted images [5].
Endoscopy usually finds a gray-white mass with smooth round surface and a unique course from the maxillary sinus to the choana. Treatment plan is based on surgery, many surgical techniques have been suggested. The ideal approach should target complete resection of the mass and yet be minimally invasive. Endoscopic sinus surgery is now used with polyp removal through the middle or inferior meatus. Recurrence rate is very rare in cases of full resection [8,9].
Conclusion
The Killian polyp is a rare benign nasal polyp more frequent in children usually originating from the maxillary sinus. CT scan can establish the diagnosis along with endoscopy. Treatment involves complete removal of the mass with low rates of recurrence.
References
- Al-Mazrou KA, Bukhari M, Al-Fayez AI. Characteristics of antrochoanal polyps in the pediatric age group. Ann Thorac Med. 2009; 4: 133-136.
- Frosini P, Picarella G, De Campora E. Antrochoanal polyp: Analysis of 200 cases. Acta Otorhinolaryngologica Italica. 2009; 29: 21-26.
- Al-Mazrou KA, Bukhari M, Al-Fayez AI. Characteristics of antrochoanal polyps in the pediatric age group. Ann Thorac Med. 2009; 4: 133-136.
- Hirshoren N, Neuman T, et al. Angiogenesis in chronic rhinosinusitis with nasal polyps and antrochoanal polyps. Inflamm Res. 2011; 60: 321-327.
- Yaman H, Yilmaz S. Evaluation and management of antrochoanal polyps. Clin Exp Otorhinolaryngol. 2010; 3: 110-114.
- Choudhury N. Hariri A, et al. Endoscopic management of antrochoanal polyp: A single UK centre’s experience. Eur Arch Otorhinolaryngol. 2015; 272: 2305-2311.
- Lee DH, Yoon TM, et al. Difference of antrochoanal polyp between children and adults. Int J Pediatr Otolaryngolol. 2016; 84: 143-146.
- Kelles M, Toplu Y. Antrochoanal polyp: Clinical presentation and retrospective comparison of endoscopic sinus surgery and endoscopic sinus surgery plus mini-Caldwell surgical procedures. J Craniofac Surg. 2014; 25: 1779-1781.
- Landsberg R, Warman M. The Rationale for Endoscopic Inferior Meatal Antrostomy. ORL. 2019; 81: 41-47.