
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Peripheral Neuropathy: A review of mechanism-based treatments with a focus on metformin as a possible choice
Niloufar Saber-Moghaddam1; Maryam Tebbi2; Morvarid Borhaninia2; Somayeh Gharibi3; Abolghasem Allahyari4; Omid Arasteh1*
1Department of Clinical Pharmacy, Faculty of Pharmacy, Mashhad University of Medical Sciences, Mashhad, Iran.
2Faculty of Pharmacy, Mashhad University of Medical Sciences, Mashhad, Iran.
3Medical Toxicology Research Center, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
4Hematology-Oncology Department, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
*Corresponding Author : Omid Arasteh
Department of clinical pharmacy, Faculty of Pharmacy, Mashhad University of Medical Sciences, Mashhad, Iran.
Tel: 098-5131801760;
Email: Arasteho@mums.ac.ir
Received : Jan 17, 2023
Accepted : Feb 03, 2023
Published : Feb 10, 2023
Archived : www.jcimcr.org
Copyright : © Arasteh O (2023).
Abstract
Purpose: Despite the troublesome nature of Peripheral Neuropathy (PN) and the possibility of irreversible complications, there is still no approved strategy for the treatment of PN. However, some atypical analgesic agents such as gabapentin, pregabalin, and duloxetine have beneficial effects. Metformin is an anti-hyperglycemic agent which is widely used for the treatment of type 2 Diabetes Mellitus (DM). In addition to its blood sugar-lowering effect, many studies have suggested that Metformin has beneficial effect in the suppression of inflammation by many mechanisms. Regarding, several studies have been conducted on the effectiveness of Metformin in the prevention or controlling the symptoms of PN. The aim of this article is to review the potential effect of Metformin as an adjuvant for the treatment of PN with a focus on diabetic neuropathy and CIPN.
Methods: In this paper, the researcher has conducted a search on PubMed and Scopus, and Web of Science for original articles and reviews published from 1993 until 2022, with the following keywords; Peripheral Neuropathy, Diabetic Neuropathy, Metformin and Post-Chemotherapy complications.
Results: We identified 79 studies at the first step of search strategy. Finally, 17 studies were included, of which 12 were animal studies and 5 were human studies.
Conclusion: In-Vitro and animal studies have shown beneficial effects of Metformin controlling the development of peripheral neuropathy. However, clinical results of using Metformin for symptomatic treatment of diabetic neuropathy is conflicting. Further clinical studies are needed to establish the effect of metformin on peripheral neuropathy.
Keywords: Peripheral neuropathy; Metformin; Inflammation; Chemotherapy-induced neuropathy.
Citation: Moghaddam NS, Tebbi M, Borhaninia M, Gharibi S, Arasteh O, et al. Peripheral neuropathy: A review of mechanism-based treatments with a focus on metformin as a possible choice. J Clin Images Med Case Rep. 2023; 4(2): 2281.
Introduction
Peripheral Neuropathy (PN) refers to the condition that the neurons of the extremities are damaged. The prevalence of all-cause peripheral neuropathy is between 6% to 50% worldwide [1]. PN usually occurs secondary to diseases or medications, among them, Diabetes Mellitus (DM) is more common. In diabetic patients, the incidence of both oxidative stress and inflammatory factors is high due to longstanding hyperglycemia, and so the development of microvascular complications such as PN is common in this population. The most important risk factors for diabetic neuropathy include age, poor glycemic control, duration of DM, and type1 versus type [2,3]. On the other hand, among drug-induced neuropathies, Chemotherapy-Induced Peripheral Neuropathy (CIPN) is an important cause of PN. The most prevalent chemotherapeutic agents associated with CIPN are platinum-based drugs, Vinka alkaloids, Taxanes, Thalidomide, and Bortezomib [4,5]. Oxaliplatin is the most common drug that can cause PN [6]. Other causes of peripheral neuropathy include advanced HIV, autoimmune diseases, congenital disorders, tumors, and metabolic diseases [7].
The clinical manifestations of PN depend on the site of involvement. Patients can experience sensory, motor, and autonomic dysfunction. However, the most common and important manifestations are paresthesia, hyperesthesia, and a sense of burning or itching in the absence of stimulants due to sensory neuronal system dysfunction. The lack of coordination and falling, bladder and bowel dysfunction, muscle weakness, and paralysis can also occur following motor and autonomic dysfunction [8,9]. Patients who develop CIPN experience more severe symptoms, involvement of feet and hand at the same time, and more rapid progression, compared to patients with diabetic neuropathy [9].
Despite the troublesome nature of PN and the possibility of irreversible complications, there is still no approved strategy for the treatment of PN [7,10]. In patients who develop diabetic neuropathy, alongside glycemic control, there are some medications that can be used as a supportive treatment for the relief of neuropathic pain and paraesthesia. Anti-epileptic drugs and anti-depressants are two groups of drugs that have been extensively used for the symptomatic treatment of diabetic neuropathy [11]. Gabapentine has been used for the treatment of chronic pain and peripheral neuropathy for decades. Duloxetine with the daily dosage of 60 mg has also proven to be as effective as Gabapentine in controlling the symptoms of PN, with fewer adverse effects [12,13]. Other drugs such as Pregabalin, Lamotrigine, Oxcarbazepine, Lacosamide, Sodium valproate, Tri Cyclic Antidepressants (TCAs), Serotonin And Nor Epinephrine Reuptake Inhibitors (SNRIs), Mexilletine, Opioids, and Tramadol also have been used in clinical trials for symptomatic treatment of diabetic neuropathy, but their effectiveness is not clearly proven [8,14-17]. Recent studies have shown that Pioglitazone can have beneficial effects in not only the prevention but also the reduction of progression of diabetic neuropathy, regarding to its anti-inflammatory effects [18-20]. Some etiology-based pharmacological treatment such as Epalrestat and Poly unsaturated fatty acid derivatives are still under study for the effectiveness on PN and safety [21-25]. For CIPN, Drugs like Fulvestrant, Minoxidil and Pirenzepin have reported to be neuroprotective [26]. Of note, TCAs and Gabapentin showed no beneficial effects in the treatment of CIPN [27].
Metformin is an anti-hyperglycemic agent which is widely used for the treatment of type 2 DM. In addition to its blood sugar-lowering effect, many studies have suggested that Metformin has beneficial effect in the suppression of inflammation by many mechanisms which are discussed later in this paper [28-32]. Regarding the anti-oxidant and anti-inflammatory activity of Metformin, several studies have been conducted on the effectiveness of metformin the prevention or controlling symptoms of peripheral neuropathy.
The aim of this article is to review the potential effect of Metformin as an adjuvant for the treatment of PN with a focus on diabetic neuropathy and CIPN.
Method
In this paper, the researcher has conducted a search on PubMed and Scopus, and Web of Science for original articles and reviews published from 1993 until 2022, with the following keywords; Peripheral Neuropathy, Diabetic Neuropathy, Metformin and Post-Chemotherapy complications. There is no limitation of time and language for identification of studies. We evaluate both preclinical and clinical studies in this manuscript.
Results
A total of 79 articles were found using the keywords. Among them, twenty articles were pre-clinical studies including studies that investigated the relationship between the mechanism of developing peripheral neuropathy and Metformin’s mechanism of action; and twelve animal studies that evaluate the effect of Metformin symptoms relief or prevention of PN. Only three of animal studies evaluated the effect of Metformin CIPN and others evaluated the effect of Metformin diabetic neuropathy. Only five articles were clinical studies, including two case study, and three comparative study that have investigated the difference in the incidence of developing PN in patients receiving Metformin and other patients. Only one clinical study evaluated the effect of Metformin on CIPN.
In animal studies Metformin was used with the dose of 100-500 mg/kg/d intra-peritoneal. Low dose Metformin (30 mg/kg) also used in two animal studies. The dose of Metformin these clinical studies varies between < 1000 mg/d to more than 2000 mg/d. A summary of these findings is listed in Table 1.
Table 1: Studies that have evaluated the effect of Metformin on PN.
| Authors | Year of publication | Study type | PN type | Metformin dosing | Sample size (each group) | Duration of treatment (days) | Results | |
|---|---|---|---|---|---|---|---|---|
| 1 | Mao-Ying QL et al | 2014 | Animal study | CIPN (Cisplatin) | 200 mg/kg /d i.p. | 27 | 14 | Metformin protects against pain and loss of tactile function in a mouse model of CIPN. The finding that met form in reduces loss of peripheral nerve endings indicates that the mechanism underlying the beneficial effects of met form in includes a neuroprotective activity. |
| 2 | Pereira et al | 2019 | Animal study | CIPN (Oxaliplatin) | 250 mg/Kg, i.p. | 40 | 30 | Metformin protected from the peripheral sensory neuropathy induced by Oxaliplatin, which was confirmed by the reduction of c-Fos and ATF3 expression, two known neuronal activation and damage markers, respectively. |
| 3 | N.W. Martinez et al. | 2020 | Animal study | CIPN (Oxaliplatin) | 250 mg/Kg, i.p. | 45 | 30 | The concomitant use of Metformin with Oxaliplatin prevented degeneration of intra-epidermal fibers, gliosis, and the altered sensitivity. |
| 4 | Sharma et al | 2012 | Animal study | Diabetic neuropathy | 120 mg/kg | 36 | 35 | Treatment with Sitagliptin combined with Metformin causes an increase in grip strength and pain sensitivity, exhibits neural protection, and reverses the alteration of biochemical parameters in rats with type 2 diabetes. |
| 5 | Ma et al | 2015 | Animal study | Diabetic neuropathy | 30 mg/kg 200 mg/kg 500 mg/kg |
60 (12 in each group) | 7 | Metformin is able to attenuate diabetes-induced hyperalgesia and allodynia, which might be associated its anti-oxidative effect through AMPK pathway. |
| 6 | Hasanvand et al | 2016 | Animal study | Diabetic neuropathy | 300 mg/kg | 18 | 45 | The activation of AMPK by metformin significantly increased the MNCV and reduced the levels of inflammatory cytokines. Administration of metformin increased the expression of p-AMPK as well as declined in the level of non-p-AMPK |
| 7 | Oliveria et al | 2016 | Animal study | Diabetic neuropathy | 100 mg/kg And 200 mg/kg | 20 | 21 | Metformin can significantly reduce neuro-inflammation and can decrease the loss of neurons in the hippocampus of diabetic animals, which can subsequently promote improvements in spatial memory. |
| 8 | Lin et al | 2018 | Animal study | Diabetic neuropathy | 200 mg/kg | 20 | 28 | The analgesic effect of Metformin against PDN is related to its inhibition of numerical increase of synaptic number in the rat spinal dorsal horn. |
| 9 | Lós D. et al. | 2019 | Animal study | Diabetic neuropathy | 100 and 200 mg/kg | 40 | 63 | Metformin prevented atrophy of myelinated axons, and reduced expression of inflammatory mediators (interleukin-1β, inducible nitric oxide synthase and nitric oxide). Metformin treatment, especially at the dose of 200 mg, protected the nerve from damages related to chronic hyperglycemia. |
| 10 | Kim et al | 2020 | Animal study | Diabetic neuropathy | 100 mg/kg/d | 40 | 90 | Metformin has beneficial pharmacological effects on the preservation of peripheral nerves in diabetic rats and its effects are comparable to those of ALA. |
| 11 | Cao et al | 2021 | Animal study | Diabetic neuropathy | Metformin alleviates diabetic mechanical allodynia via activation of AMPK signaling pathway in L4-6 DRGs of diabetic rats, which might be mediated by the down regulation of NF-κ B, and this providing certain basis for Met form in to become a potential drug in the clinical treatment of diabetic neuropathic pain. | |||
| 12 | Ma et al | 2022 | Animal study | Diabetic neuropathy | 100 mg/kg/d | 40 | 30 | Metformin is able to accelerate sciatic nerve repair after transection injury under diabetic conditions, showing the therapeutic potential of metformin in the management of nerve injuries during diabetes mellitus. |
| 13 | Bell D. | 2010 | Case report | Diabetic neuropathy | 1000 mg BD | 1 | 90 | Metformin-induced vitamin B12 deficiency causing neuropathy. |
| 14 | El-fatatry et al. | 2018 | RCT | CIPN Oxaliplatin | 500 mg TDS | 55 | 12 cycles of chemotherapy | At the end of the 12th cycle, there were less patients with grade 2 and 3 neuropathy in metformin arm as compared to control arm. the mean pain score in metformin arm was significantly lower than those of control arm. |
| 15 | Farooq et al | 2022 | RCT | Diabetic neuropathy | 500 mg TDS | There was significant negative correlation between cumulative metformin dose and vitamin B12 level Metformin use is associated with vitamin B12 deficiency and clinical neuropathy in Type 2 diabetes patients. | ||
| 16 | Hashem M et al | 2021 | RCT | Diabetic neuropathy | < 1000 mg/d to >2000 mg/d | 150 | 180 | Diabetics treated with metformin for prolonged duration and higher doses were associated with lower cobalamin and more severe DPN. |
| 17 | Wile et al | 2009 | Case study | Diabetic neuropathy | Mean cumulative exposure 3385 g | 3 | >180 | Metformin exposure may be an iatrogenic cause for exacerbation of peripheral neuropathy in patients with type 2 diabetes. |
Discussion
To date, many drugs have been used for the treatment of PN of all causes. Among them, Duloxetine and Gabapentin seemed to be effective in controlling the symptoms of Diabetic Neuropathy but not CIPN. The beneficial effect of other drugs such as TCAs, SNRIs, Opioids and Tramadol is not yet proven. Regarding the anti-oxidant and anti-inflammatory activity of Metformin, several studies have been conducted on the effectiveness of metformin in the prevention or controlling symptoms of PN. In the following, we have reviewed the pre-clinical and clinical studies that investigated the effect of Metformin in the treatment of PN.
Pre-clinical studies on the treatment of PN
Many therapeutic strategies have been evaluated for the treatment of PN based on its mechanism of developing. Among them, Metformin has a particular place due to its anti-inflammatory effects along with its proven hypoglycemic effects.
Kim et al mentioned that Metformin can play a beneficial role in the prevention of diabetic neuropathy, they also suggested that the effect is comparable to Alpha lipoic acid. Furthermore, Metformin can reduce Reactive Oxygen Species (ROS), Nitric Oxide (NO), and other oxidative stress markers which express due to hyperglycemia, or the administration of chemotherapeutic agents [33].
Studies have shown the anti-inflammatory effect of Metformin in neurons by activating AMPK signaling pathway and inhibition of m TORC1 pathway. They also reported that Metformin can reduce the expression of inflammatory mediators such as TNF-alpha, Interleukin 10 (IL-10) and IL-6 [34-41]. Ma et al reported that Metformin can reduce the symptoms of diabetic neuropathy such as allodynia and hyperalgesia in Streptozocin (STZ) induced diabetic rats [42]. Further studies have suggested that higher doses of Metformin have efficiently reduced the inflammatory cytokines expression and accelerate the nerve repair in STZ-induced diabetic rats [43,44]. Sharma et al reported that Metformin can relief diabetic neuropathy symptoms, exhibit neuroprotective effects and reduce inflammatory factors when used in combination with Sitagliptin in STZ/nicotinamide-induced diabetic rats [45].
Studies have mentioned that addition of Metformin to Oxaliplatin can prevented CIPN [46,47]. Mao et al confirmed the result of previous studies and mentioned that Metformin has protective effect against Paclitaxel and Cisplatin induced PN [48].
Clinical studies on the treatment of PN
There are limited clinical studies on the treatment of all-cause PN. In diabetic patients, glycemic control with BS lowering agents such as Metformin is the best known strategy for the prevention of developing PN [11]. However, the outcomes of studies, using Metformin as symptomatic treatment of diabetic neuropathy, is not consistent with pre-clinical studies. Many studies have mentioned that vitamin B12 deficiency caused by Metformin use in diabetic patients can cause and even worsen diabetic neuropathy and should be carefully noticed in diabetic population [49-54].
Hashem et al mentioned that using Metformin could worsen diabetic neuropathy in patients with type 2 DM [52]. Luo et al also mentioned that Metformin administration in type 2 DM patients was associated with higher incidence of developing diabetic PN. They named prolong use, higher cumulative dose of Metformin and male sex as the major risk factors for developing PN [53].
El-fatatry et al mentioned that Metformin has neuroprotective effects in Oxaliplatin recipients [55].
Mechanisms of peripheral neuropathy development
Oxidative stress and inflammation are the cornerstone of developing PN, especially in diabetic patients [8,15,56,57]. Prolonged hyperglycemia causes the activation of inflammatory cascades and an increase in the level of inflammatory cytokines as well as higher formation of oxidative metabolic end-products which can cause direct neuronal injury and hypoxic damage due to vascular injury [57]. In addition to inflammatory cytokines, recent studies have mentioned that the increase or depletion of some cellular factors which are released from other tissues such as muscle and skin also play a role in diabetic neuropathy, that neurotrophine is a good example of them [58-61]. Another mechanism for developing diabetic neuropathy is the production of chimeric cells from bone marrow of diabetic patients which can cause neuronal injury [6]. Involved molecular and cellular pathways are listed in Table 2.
Table 2: Cellular mechanisms of the development of diabetic neuropathy.
| Pathway/ Response | Activity | Result | Drug available |
|---|---|---|---|
| Aldose reductase pathway | Increased | Polyol flux Increased Reactive Oxygen Species (ROS) |
Epalrestat |
| Advanced Glycation End-Products (AGE)/receptor for AGE (RAGE) reactions | Increased | Increased ROS Increased iNOS activity in neurons and vessels Reduced myelinated nerve fiber density induction of apoptosis |
Aminoguanidine |
| Release of Tumor Necrosis Factor (TNF)-α activate transcription of Nuclear Factor-Κb (NF-κB) | |||
| Oxidative stress | Increased | Induction of apoptosis Impaired neurotrophic support Poly ADP-Ribose Polymerase (PARP) activation |
α-lipoic acid |
| PKC activation | Reduce | Increase of PKC-β in vessels Decrease of PKC-α in neurons |
No drug is available |
| Pro-inflammatory Processes | Increase | Increased TNF-α Increased ILs Increase in cyclooxygenase (COX)-2 Activated protein (MAP)-kinase NF-κ B is activated |
N-acetylcysteine Pioglitazone |
| Cellular and Trophic Factors | Reduce | Increased apoptosis | No drug is available |
The mechanism of developing CIPN depends on the chemotherapeutic regimen, but it is mainly similar to the diabetic neuropathy, including oxidative stress and inflammatory cascade activation in the nerve tissues [9,26,63]. Platinium-based drugs such as cisplatin can cause alteration in neuronal excitation via releasing ROS, resulting in calcium hemostasis dysregulation, apoptotic changes in neurons and axonal degeneration. Cisplatin can also cause neuro-inflammation by stimulating immune system and hyper excitability of peripheral neurons [64]. Furthermore, Platinium metabolites and byproducts such as oxalate can accumulate in neurons and initiate neurotoxicity [65-67]. Pro- inflammatory cytokines such as TNF a, IL 1b and IL-6 also play a vital role in the development of CIPN. Inflammation can change ion channels activity, sensitize nociceptors and result in the development of neuronal damage [68,69]. In addition to named mechanisms, Thalidomide can cause neurotoxicity via its anti-angiogenesis effect, resulting in nerve tissue hypoxia and ischemia [70,71]. The mechanism of developing CIPN by Paclitaxel is the same as Cisplatin, by addition of the direct neurotoxic effects of that on axons and peripheral nerve damage [9,72,73]. Older ages, other comorbidities such as diabetes and lower levels of vitamin D is known risk factors for developing CIPN [9,74].
Possible resolutions for the treatment of PN
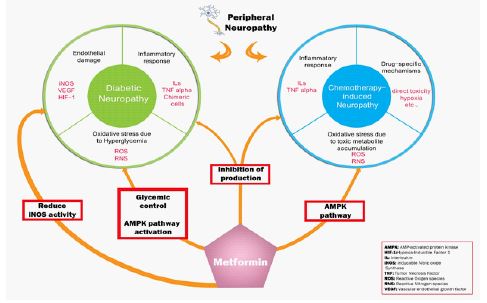
In this study, the researcher has explored studies that have been published since 1993 to 2022, to demonstrate the therapeutic options for the treatment of PN. In patients with diabetic neuropathy, glycemic control is the mainstay of the treatment of PN. Some drugs such as Duloxetine and Pregabalin, also have a place in relieving symptoms [8]. Metformin is one of the most convenient anti-hyperglycemic agents worldwide. In addition to its beneficial effect in reducıng BS and suppressing almost all cellular pathways that are involved in the development of diabetic neuropathy, studies have shown that Metformin can be effective in reducing symptoms of neuropathy in both diabetic neuropathy and CIPN due to its direct anti-inflammatory effects [33,46-48,75]. Metformin plays its neuroprotective role by reducing I NOS pathway activity, reduction of pro-inflammatory cytokines such as TNF, IL6, IL10, and m TOR inhibitory effect [34,35,37,38,40,41]. Figure 1 shows the mechanisms that Metformin can affect diabetic neuropathy and CIPN.
However, there are concerns about using Metformin as an adjuvant for the treatment of PN. To date, many clinical studies suggested that long-term use of Metformin, especially over 5 years and higher cumulative dose of Metformin is associated with vitamin B12 deficiency, which can cause progression of central and peripheral neuropathy [49-54]. Contrary to initial disappointing results, Russo et al mentioned that in type 2 DM patients who received Metformin for at least 6 months, vitamin B12 deficiency was just mild and didn’t have a relationship with developing diabetic neuropathy [76]. Fakkar et al confirmed the previous study and mentioned that despite the lower levels of vit B12 in Metformin recipients, it is not associated with higher incidence of developing PN [77]. The last systematic review published in could not analyze the effect of Metformin on PN in diabetic patients due to the lack of data [78].
Limitations
Lack of a large clinical trial to evaluate the effectiveness of Metformin in controlling the symptoms of all cause peripheral neuropathy is by far the most significant limitation of this study.
Conclusion
This review is aimed to evaluate the effect of Metformin on the treatment of diabetic neuropathy and chemotherapy-induced neuropathy. In-Vitro and animal studies have shown beneficial effects of Metformin in controlling the development and progression of diabetic neuropathy and chemotherapy induced neuropathy. However, clinical results of using Metformin alone or as an adjuvant to other drugs for symptomatic treatment of diabetic neuropathy is conflicting. Further clinical studies are required indeed to make a strong decision about the effectiveness of Metformin in the treatment of all cause peripheral neuropathy.
Declarations
Source of funding: No funding was received for preparation of this review.
Conflict of interests: The authors have no competing interests to declare.
Authors’ contributions: To write this manuscript, all of the writers have role. N.S. and M.T. and M.B wrote the first draft of manuscript. S. G and A.A revised the manuscript. Finally, O.A has proposed the main idea of the paper and also did the scientific revision of the article.
Availability of data and materials: The access to different datasets was through Mashhad University of Medical Sciences.
References
- Hicks CW, Selvin E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr Diab Rep. 2019; 19: 86.
- Sun J, Wang Y, Zhang X, Zhu S, He H. Prevalence of peripheral neuropathy in patients with diabetes: A systematic review and meta-analysis. Primary Care Diabetes. 2020; 14: 435-444.
- Vinik AI, Nevoret ML, Casellini C, Parson H. Diabetic neuropathy. Endocrinol Metab Clin North Am. 2013; 42: 747-787.
- Derman BA, Davis AM. Recommendations for Prevention and Management of Chemotherapy-Induced Peripheral Neuropathy. JAMA. 2021; 326: 1058-1059.
- Piccolo J, Kolesar JM. Prevention and treatment of chemotherapy-induced peripheral neuropathy. Am J Health Syst Pharm. 2014; 71: 19-25.
- Gebremedhn EG, Shortland PJ, Mahns DA. The incidence of acute oxaliplatin-induced neuropathy and its impact on treatment in the first cycle: A systematic review. BMC Cancer. 2018; 18: 410.
- Pisciotta C, Shy ME. Neuropathy. Handb Clin Neurol. 2018; 148: 653-665.
- Callaghan BC, Cheng HT, Stables CL, Smith AL, Feldman EL. Diabetic neuropathy: Clinical manifestations and current treatments. Lancet Neurol. 2012; 11: 521-534.
- Zajączkowska R, Kocot-Kępska M, Leppert W, Wrzosek A, Mika J, Wordliczek J, et al. Mechanisms of Chemotherapy-Induced Peripheral Neuropathy. Int J Mol Sci. 2019; 20.
- Baron R. Peripheral neuropathic pain: from mechanisms to symptoms. The Clinical journal of pain. 2000; 16: S12-20.
- Várkonyi T, Kempler P. Diabetic neuropathy: New strategies for treatment. Diabetes, Obesity and Metabolism. 2008; 10: 99-108.
- Jiang L, Xiong Y, Cui J. Comparison of the Efficacy and Safety of Duloxetine and Gabapentin in Diabetic Peripheral Neuropathic Pain: A Meta-Analysis. Contrast Media & Molecular Imaging. 2022; 2022: 4084420.
- Lunn MP, Hughes RA, Wiffen PJ. Duloxetine for treating painful neuropathy or chronic pain. Cochrane Database Syst Rev. 2009: Cd007115.
- Feldman EL, Callaghan BC, Pop-Busui R, Zochodne DW, Wright DE, et al. Diabetic neuropathy. Nat Rev Dis Primers. 2019; 5: 41.
- Singh R, Kishore L, Kaur N. Diabetic peripheral neuropathy: current perspective and future directions. Pharmacol Res. 2014; 80: 21-35.
- Bayram EH, Sezer AD, Elçioğlu HKb. Diabetic neuropathy and treatment strategy-new challenges and applications. Smart Drug Delivery System. 2016; 2: 24-35.
- Jarvis B, Coukell AJ. Mexiletine. A review of its therapeutic use in painful diabetic neuropathy. Drugs. 1998; 56: 691-707.
- Du Y, Tang J, Li G, Berti-Mattera L, Lee CA, Bartkowski D, et al. Effects of p38 MAPK inhibition on early stages of diabetic retinopathy and sensory nerve function. Invest Ophthalmol Vis Sci. 2010; 51: 2158-2164.
- Tomlinson DR. Mitogen-activated protein kinases as glucose transducers for diabetic complications. Diabetologia. 1999; 42: 1271-1281.
- Yamagishi S, Ogasawara S, Mizukami H, Yajima N, Wada R, et al. Correction of protein kinase C activity and macrophage migration in peripheral nerve by pioglitazone, peroxisome proliferator activated-gamma-ligand, in insulin-deficient diabetic rats. J Neurochem. 2008; 104: 491-499.
- Goto Y, Hotta N, Shigeta Y, Sakamoto N, Kikkawa R. Effects of an aldose reductase inhibitor, epalrestat, on diabetic neuropathy. Clinical benefit and indication for the drug assessed from the results of a placebo-controlled double-blind study. Biomed Pharmacother. 1995; 49: 269-277.
- Cameron NE, Cotter MA. Potential therapeutic approaches to the treatment or prevention of diabetic neuropathy: evidence from experimental studies. Diabet Med. 1993; 10: 593-605.
- Hotta N, Kawamori R, Atsumi Y, Baba M, Kishikawa H, et al. Stratified analyses for selecting appropriate target patients with diabetic peripheral neuropathy for long-term treatment with an aldose reductase inhibitor, epalrestat. Diabet Med. 2008; 25: 818-825.
- Obrosova IG. Diabetes and the peripheral nerve. Biochim Biophys Acta. 2009; 1792: 931-940.
- Pfeifer MA, Schumer MP, Gelber DA. Aldose Reductase Inhibitors: The End of an Era or the Need for Different Trial Designs? Diabetes. 1997; 46 : S82-S89.
- Yamamoto S, Egashira N. Drug Repositioning for the Prevention and Treatment of Chemotherapy-Induced Peripheral Neuropathy: A Mechanism- and Screening-Based Strategy. Frontiers in Pharmacology. 2021; 11.
- Hu LY, Mi WL, Wu GC, Wang YQ, Mao-Ying QL. Prevention and Treatment for Chemotherapy-Induced Peripheral Neuropathy: Therapies Based on CIPN Mechanisms. Curr Neuropharmacol. 2019; 17: 184-196.
- Saisho Y. Metformin and Inflammation: Its Potential Beyond Glucose-lowering Effect. Endocrine, Metabolic & Immune Disorders - Drug Targets(Formerly Current Drug Targets - Immune, Endocrine & Metabolic Disorders). 2015; 15: 196-205.
- Bharath LP, Nikolajczyk BS. The intersection of metformin and inflammation. American Journal of Physiology-Cell Physiology. 2021; 320: C873-C879.
- Correia S, Carvalho C, Santos MS, Seiça R, Oliveira CR, Moreira PI, et al. Mechanisms of action of metformin in type 2 diabetes and associated complications: an overview. Mini Rev Med Chem. 2008; 8: 1343-1354.
- Davis BJ, Xie Z, Viollet B, Zou MH. Activation of the AMP-activated kinase by antidiabetes drug metformin stimulates nitric oxide synthesis in vivo by promoting the association of heat shock protein 90 and endothelial nitric oxide synthase. Diabetes. 2006; 55: 496-505.
- Majithiya JB, Balaraman R. Metformin reduces blood pressure and restores endothelial function in aorta of streptozotocin-induced diabetic rats. Life Sci. 2006; 78: 2615-2624.
- Kim SH, Park TS, Jin HY. Metformin Preserves Peripheral Nerve Damage with Comparable Effects to Alpha Lipoic Acid in Streptozotocin/High-Fat Diet Induced Diabetic Rats. Diabetes Metab J. 2020; 44: 842-853.
- Asiedu MN, Dussor G, Price TJ. Targeting AMPK for the Alleviation of Pathological Pain. Exp Suppl. 2016; 107: 257-285.
- Baeza-Flores GDC, Guzmán-Priego CG, Parra-Flores LI, Murbartián J, Torres-López JE, et al. Metformin: A Prospective Alternative for the Treatment of Chronic Pain. Frontiers in Pharmacology. 2020; 11.
- Cao XJ, Wu R, Qian HY, Chen X, Zhu HY, et al. Metformin attenuates diabetic neuropathic pain via AMPK/NF-κB signaling pathway in dorsal root ganglion of diabetic rats. Brain Research. 2021; 1772: 147663.
- Demaré S, Kothari A, Calcutt NA, Fernyhough P. Metformin as a potential therapeutic for neurological disease: Mobilizing AMPK to repair the nervous system. Expert Rev Neurother. 2021; 21: 45-63.
- Hasanvand A, Amini-Khoei H, Hadian MR, Abdollahi A, Tavangar SM, et al. Anti-inflammatory effect of AMPK signaling pathway in rat model of diabetic neuropathy. Inflammopharmacology. 2016; 24: 207-219.
- Lin JY, He YN, Zhu N, Peng B. Metformin attenuates increase of synaptic number in the rat spinal dorsal horn with painful diabetic neuropathy induced by type 2 diabetes: A stereological study. Neurochemical Research. 2018; 43: 2232-229.
- Oliveira WH, Nunes AK, França MER, Santos LA, Lós DB, et al. Effects of metformin on inflammation and short-term memory in streptozotocin-induced diabetic mice. Brain Research. 2016; 1644: 149-160.
- Price TJ, Das V, Dussor G. Adenosine Monophosphate-activated Protein Kinase (AMPK) Activators For the Prevention, Treatment and Potential Reversal of Pathological Pain. Curr Drug Targets. 2016; 17: 908-920.
- Ma J, Yu H, Liu J, Chen Y, Wang Q, et al. Metformin attenuates hyperalgesia and allodynia in rats with painful diabetic neuropathy induced by streptozotocin. European Journal of Pharmacology. 2015; 764: 599-606.
- Lós DB, Oliveira WH, Duarte-Silva E, Sougey WWD, Freitas E, et al. Preventive role of metformin on peripheral neuropathy induced by diabetes. Int Immunopharmacol. 2019; 74: 105672.
- Ma J, Liu J, Chen Y, Yu H, Xiang L. Metformin Promotes Axonal Regeneration and Functional Recovery in Diabetic Rat Model of Sciatic Nerve Transection Injury. NeuroSci. 2022; 3: 366-375.
- Sharma AK, Sharma A, Kumari R, Kishore K, Sharma D, et al. Sitagliptin, sitagliptin and metformin, or sitagliptin and amitriptyline attenuate streptozotocin-nicotinamide induced diabetic neuropathy in rats. Journal of Biomedical Research. 2012; 26: 200-210.
- Martinez NW, Sánchez A, Diaz P, Broekhuizen R, Godoy J, Mondaca S, et al. Metformin protects from oxaliplatin induced peripheral neuropathy in rats. Neurobiol Pain. 2020; 8: 100048.
- Pereira AF, Pereira LMS, Silva CMP, Freitas Alves BW, Barbosa JS, et al. Metformin reduces c-Fos and ATF3 expression in the dorsal root ganglia and protects against oxaliplatin-induced peripheral sensory neuropathy in mice. Neurosci Lett. 2019; 709: 134378.
- Mao-Ying QL, Kavelaars A, Krukowski K, Huo XJ, Zhou W, Price TJ, et al. The anti-diabetic drug metformin protects against chemotherapy-induced peripheral neuropathy in a mouse model. PLoS One. 2014; 9: e100701.
- Bell DSH. Metformin-induced vitamin B12 deficiency presenting as a peripheral neuropathy. Southern medical journal. 2010; 103: 265-267.
- Bell DSH. Metformin-induced vitamin B12 deficiency can cause or worsen distal symmetrical, autonomic and cardiac neuropathy in the patient with diabetes. Diabetes, Obesity and Metabolism. 2022; 24: 1423-1428.
- Farooq MD, Tak FA, Ara F, Rashid S, Mir IA. Vitamin B12 Deficiency and Clinical Neuropathy with Metformin Use in Type 2 Diabetes. Journal of Xenobiotics. 2022; 12: 122-130.
- Hashem MM, Esmael A, Nassar AK, El-Sherif M. The relationship between exacerbated diabetic peripheral neuropathy and metformin treatment in type 2 diabetes mellitus. Sci Rep. 2021; 11: 1940.
- PAN Q, LUO J, GUO L. 467-P: The Relationship between Diabetic Peripheral Neuropathy and Metformin Treatment in Type 2 Diabetes Mellitus. Diabetes. 2022; 71.
- Wile DJ, Toth C. Association of Metformin, Elevated Homocysteine, and Methylmalonic Acid Levels and Clinically Worsened Diabetic Peripheral Neuropathy. Diabetes Care. 2009; 33: 156-161.
- El-Fatatry BM, Ibrahim OM, Hussien FZ, Mostafa TM. Role of metformin in oxaliplatin-induced peripheral neuropathy in patients with stage III colorectal cancer: Randomized, controlled study. Int J Colorectal Dis. 2018; 33: 1675-1683.
- Dewanjee S, Das S, Das AK, Bhattacharjee N, Dihingia A, Dua TK, et al. Molecular mechanism of diabetic neuropathy and its pharmacotherapeutic targets. Eur J Pharmacol. 2018; 833:472-523.
- Yagihashi S, Yamagishi S, Wada R. [Perspective for the treatment of diabetic neuropathy: translation from molecular studies to bedside]. Rinsho Shinkeigaku. 2005; 45: 966-968.
- Anand P, Terenghi G, Warner G, Kopelman P, Williams-Chestnut RE. The role of endogenous nerve growth factor in human diabetic neuropathy. Nat Med. 1996; 2: 703-707.
- Andreassen CS, Jakobsen J, Flyvbjerg A, Andersen H. Expression of neurotrophic factors in diabetic muscle-relation to neuropathy and muscle strength. Brain. 2009; 132: 2724-2733.
- Tomlinson DR, Fernyhough P, Diemel LT. Neurotrophins and peripheral neuropathy. Philos Trans R Soc Lond B Biol Sci. 1996; 351: 455-462.
- Tomlinson DR, Fernyhough P, Diemel LT. Role of neurotrophins in diabetic neuropathy and treatment with nerve growth factors. Diabetes. 1997; 46 : S43-49.
- Busik JV, Tikhonenko M, Bhatwadekar A, Opreanu M, Yakubova N, Caballero S, et al. Diabetic retinopathy is associated with bone marrow neuropathy and a depressed peripheral clock. J Exp Med. 2009; 206: 2897-2906.
- Hu LY, Mi WL, Wu GC, Wang YQ, Mao Ying QL. Prevention and Treatment for Chemotherapy-Induced Peripheral Neuropathy: Therapies Based on CIPN Mechanisms. Current neuropharmacology. 2019; 17: 184-196.
- McKeage MJ, Hsu T, Screnci D, Haddad G, Baguley BC. Nucleolar damage correlates with neurotoxicity induced by different platinum drugs. Br J Cancer. 2001; 85: 1219-1225.
- Jaggi AS, Singh N. Mechanisms in cancer-chemotherapeutic drugs-induced peripheral neuropathy. Toxicology. 2012; 291: 1-9.
- Kober KM, Olshen A, Conley YP, Schumacher M, Topp K, et al. Expression of mitochondrial dysfunction-related genes and pathways in paclitaxel-induced peripheral neuropathy in breast cancer survivors. Mol Pain. 2018; 14: 1744806918816462.
- Viatchenko-Karpinski V, Ling J, Gu JG. Down-regulation of Kv4.3 channels and a-type K(+) currents in V2 trigeminal ganglion neurons of rats following oxaliplatin treatment. Mol Pain. 2018; 14: 1744806917750995.
- Di Cesare Mannelli L, Pacini A, Micheli L, Tani A, Zanardelli M, et al. Glial role in oxaliplatin-induced neuropathic pain. Exp Neurol. 2014; 261: 22-33.
- Lees JG, Makker PG, Tonkin RS, Abdulla M, Park SB, Goldstein D, et al. Immune-mediated processes implicated in chemotherapy-induced peripheral neuropathy. Eur J Cancer. 2017; 73: 22-29.
- Jongen JL, Broijl A, Sonneveld P. Chemotherapy-induced peripheral neuropathies in hematological malignancies. J Neuro Oncol. 2015; 121: 229-237.
- Tamilarasan KP, Kolluru GK, Rajaram M, Indhumathy M, Saranya R, Chatterjee S, et al. Thalidomide attenuates nitric oxide me diated angiogenesis by blocking migration of endothelial cells. BMC Cell Biol. 2006; 7: 17.
- Gornstein EL, Schwarz TL. Neurotoxic mechanisms of paclitaxel are local to the distal axon and independent of transport defects. Exp Neurol. 2017; 288: 153-166.
- Sahenk Z, Barohn R, New P, Mendell JR. Taxol neuropathy. Electrodiagnostic and sural nerve biopsy findings. Arch Neurol. 1994; 51: 726-729.
- Wang J, Udd KA, Vidisheva A, Swift RA, Spektor TM, et al. Low serum vitamin D occurs commonly among multiple myeloma patients treated with bortezomib and/or thalidomide and is associated with severe neuropathy. Support Care Cancer. 2016; 24: 3105-3110.
- Burcelin R. The antidiabetic gutsy role of metformin uncovered? Gut. 2014; 63: 706.
- Russo GT, Giandalia A, Romeo EL, Scarcella C, Gambadoro N, et al. Diabetic neuropathy is not associated with homocysteine, folate, vitamin B12 levels, and MTHFR C677T mutation in type 2 diabetic outpatients taking metformin. Journal of Endocrinological Investigation. 2016; 39: 305-314.
- Fakkar NFH, Marzouk D, Allam MF, Fouad MM, Aboromia MM, et al. Association between vitamin B12 level and clinical peripheral neuropathy in type 2 diabetic patients on metformin therapy. The Egyptian Journal of Neurology, Psychiatry and Neurosurgery. 2022; 58: 46.
- Gerardo González-González J, Cesar Solis R, Díaz González-Colmenero A, Raygoza-Cortez K, Moreno-Peña PJ, et al. Effect of metformin on microvascular outcomes in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Research and Clinical Practice. 2022; 186: 109821.