
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Median incisional hernia and double parastomal hernia repair with retromuscular prosthetic biomaterial mesh using SMART technique (Stapled Mesh Stoma Reinforcement Technique) after pelvic exenteration due to cancer
Pierre-Yves Blanc*; Bertrand Le Roy; Laura Ornella Perotto
Saint-Etienne University Hospital, Visceral and Digestive Surgery Unit – F-42055 Saint-Etienne Cedex, France.
*Corresponding Author : Pierre-Yves Blanc
Saint-Etienne University Hospital, Visceral and Digestive Surgery Unit – F-42055 Saint-Etienne Cedex, France.
Email: pierre.yves.blanc.pro@gmail.com
Received : Jan 12, 2023
Accepted : Feb 07, 2023
Published : Feb 14, 2023
Archived : www.jcimcr.org
Copyright : © Blanc PY (2023).
Abstract
Patient aged 64 with parastomal hernia on a terminal colostomy and a Bricker ileal conduit following pelvic exenteration in the context of a locally advanced low rectal adenocarcinoma. Underwent in 2021 a first median incisional hernia using an intraperitoneal biomaterial mesh, reoperated one year later, when appeared a symptomatic parastomal hernia at stomial sites and next to the median laparotomy scar. The decision in favour of a double parastomal hernia repair using SMART technique with retromuscular prosthetic biomaterial mesh was then taken.
Keywords: Incisional hernia; Parastomal hernia; Colostomy; Bricker; Ileal conduit; SMART (Stapled Mesh stoma Reinforcement Technique).
Citation: Blanc PV, Le Roy B, Perotto LO. Median incisional hernia and double parastomal hernia repair with retromuscular prosthetic biomaterial mesh using SMART technique (Stapled Mesh Stoma Reinforcement Technique) after pelvic exenteration due to cancer. J Clin Images Med Case Rep. 2023; 4(2): 2286.
Case report
Patient aged 64 with obesity, underwent a pelvic exenteration surgery in 2019 due to ypT3N0M0 low rectal adenocarcinoma after neoadjuvant chemoradiotherapy.
A symptomatic median incisional hernia and asymptomatic parastomal hernia appeared earlier in 2021 on grade II colostomy [1]. Patient underwent a first incisional hernia repair surgery where intraperitoneal biomaterial mesh covered both stomial openings. One year after this surgery, patient showed a recurrent median herniation and 2 grade II parastomal hernias (Figure 1), symptomatic.
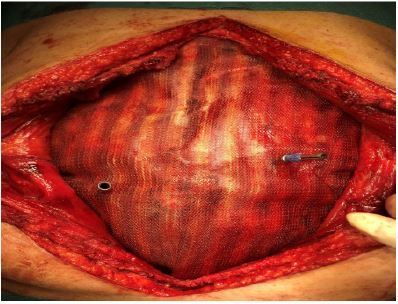
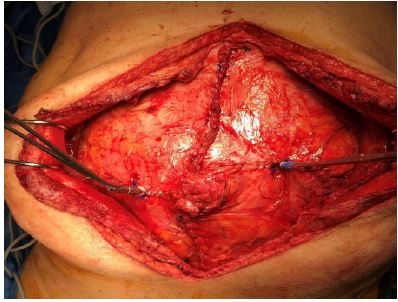
A second surgery was performed in 2022 with retromuscular prosthetic biomaterial mesh plasty using the SMART technique [2]. The procedure was a median open surgery with disintertion of the 2 stomata identified by suture. Posterior aponeurosis was closed with bursa placement on circular stapler anvils with diameter 28 mm (colostomy) and diameter 26 mm (urostomy). We used a double-sided biomaterial mesh measuring 30 x 35 cm, in a retromuscular position (Figure 2). The anterior aponeurosis was closed after anvils were brought out through both aponeuroses and the mesh (Figure 3). Circular stapling allowed us to create a stomial opening through apeunoroses and through the mesh (Figure 4). The two stomia were brought out quite easily. A urinary catheter was left in place in urostomy to make postoperative diurese easier.
The development of an infected collection due to the open surgery was among main consequences. It was treated by probabilistic antibiotic therapy over 12 weeks by partial disunity of the two stomata with subcutaneous abscesses requiring controlled wound healing. Patient left the hospital 20 days later. Wound healing was completed within 3 months. No recurrence hernia after six months of follow up. In this case precisely, the use of a synthetic biomaterial mesh in a contaminated environment seems appropriate [3] together with postoperative infection management by antibiotics and local treatment.


References
- Śmietański M, Szczepkowski M, Alexandre JA, Berger D, Bury K, Conze J, et al. European. Hernia Society classification of parastomal hernias. Hernia. 2014; 18: 1-6.
- Williams NS, Nair R, Bhan C. Stapled mesh stoma reinforcement technique (SMART) – A procedure to prevent parastomal herniation. Ann R Coll Surg Engl. 2011; 93: 169.
- Vauclair E, Bert M, Facy O, Cheynel N, Rat P, Ortega-Deballon P, et al. What results can be expected one year after complex incisional hernia repair with biosynthetic mesh. Visceral Surgery Journ. 2021; 158: 118-124.