
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Insulinoma: 4 case reports
Maram Ben Salem*; Marwa Chiboub; Manel Jemel; Hajer Kandara; Ines Kammoun
Department of Endocrinology, National Institute of Nutrition, Tunis, Tunisia.
*Corresponding Author : Maram Ben Salem
Department of Endocrinology, National Institute of Nutrition, Tunis, Tunisia.
Email: maram-bs@hotmail.com
Received : Jan 19, 2023
Accepted : Feb 08, 2023
Published : Feb 15, 2023
Archived : www.jcimcr.org
Copyright : © Salem MB (2023).
Abstract
Insulinoma is a rare variety of endocrine neoplasm and is usually benign, solitary, and small in size. It is responsible of endogenous insulin secretion resulting in development of symptoms of hypoglycemia. Diagnosis of insulinomas can be challenging. We report 4 cases of insulinoma that were diagnosed and managed in the year 2022. Three women and one man, with a mean age of 61.5 years. The diagnosis was confirmed biochemically in all cases and tumors were located preoperatively in three cases. In the fourth case, intraoperative diagnosis was made. Enucleation was performed in all the cases and the tumors were confirmed to be benign after histopathology in the four cases.
Keywords: Insulinoma; Imaging; Surgery; Recurrence.
Citation: Salem MB, Chiboub M, Jemel M, Kandara H, Kammoun I. Insulinoma: 4 case reports. J Clin Images Med Case Rep. 2023; 4(2): 2287.
Background
Insulinoma is a rare pancreatic endocrine tumor that results in excessive endogenous insulin secretion. It occurs in 0.5-5 people per million of the general population [1]. Insulinomas have a male-to-female ratio of 2:3 and can occur at any age [2]. 90% of insulinomas are sporadic, however 10% may occur as part of multiple endocrine neoplasia type 1 [3]. Early diagnosis of the disease is essential to prevent occurrence of lethal hypoglycemia. Non-invasive imaging procedures, such as computed tomography and magnetic resonance imaging, are used when a diagnosis of insulinoma has been made to localize the source of pathological insulin secretion [4,5]. Invasive modalities, such as endoscopic ultrasonography and arterial stimulation venous sampling, are highly accurate in the preoperative localization of insulinomas and have frequently been shown to be superior to non-invasive localization techniques [6-8]. Treatment of insulinomas consist in surgical resection of the tumor.
Case presentation
We report four cases of insulinomas diagnosed in the same year of 2022. Three women and one man aged respectively 76, 68, 60 and 42 years-old. All patients presented a long history of various adrenergic symptoms of hypoglycemia and one patient presented signs of neuroglycopenia including behavior changes and confusion. The mean duration of the symptoms was 8.7 years. Three patients presented spontaneous hypoglycemia with a mean plasma glucose levels of 0.28 g/l concomitant with inappropriately high insulin and C-peptide levels. The positive diagnosis was made in one patient after an 8 hour fasting test (Table 1).
Table 1: Biochemical findings allowing positive diagnosis of insulinoma in the 4 cases.
| Glucose plasma level (g/l) | Insulin plasma level (μUI/ml) | C-peptide plasma level (ng/ml) | |
|---|---|---|---|
| Case 1 | 0.20 | 46 | 12.1 |
| Case 2 | 0.36 | 60 | 9.7 |
| Case 3 | 0.27 | 16 | 6.9 |
| Case 4 | 0.32 | 22 | 7.6 |
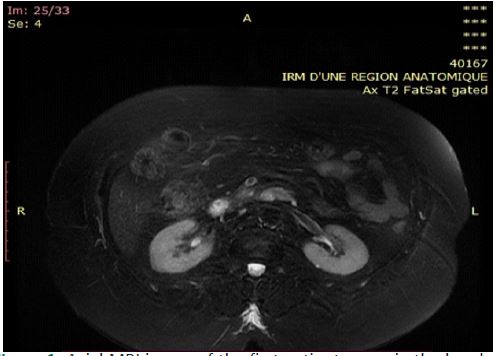
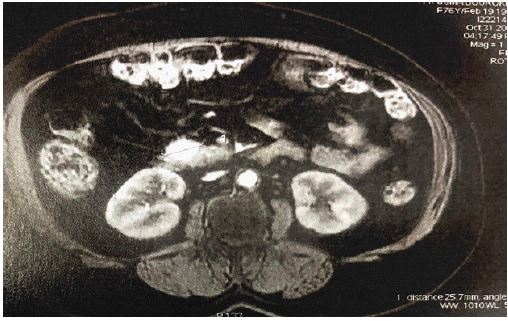
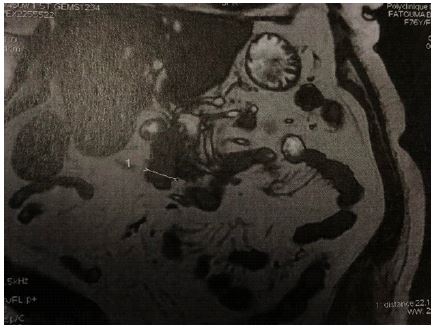
The tumors were located preoperatively in 3 cases using pancreatic MRI which have objective a unique nodule in all cases with a mean size of 20 mm (Figures 1,2 and 3). In one case, abdominal CT scan, pancreatic MRI and endoscopic ultrasonography were practiced but the tumor was not located.
All patients underwent laparotomies and the tumors were localized peroperatively. Enucleation of the nodules were practiced and all the tumors turned out to be benign after histo pathological examination. Symptoms disappeared postoperatively in all cases and the glucose plasma levels were normal during a mean follow up duration of 5 months.
Discussion
Diagnosis of insulinoma remains challenging regarding the variety of symptoms that may reveal the diagnosis. The median duration of symptoms before diagnosis is variable and may reach several months to several years in some cases [9]. The diagnosis of insulinoma remains difficult, in fact, symptoms are delayed due to the adaptations by the central nervous system to chronic hypoglycemia [10]. The cornerstone of the diagnosis is the Whipple’s triad: hypoglycemia (plasma glucose level < 0.5 g/l), neuroglycopenic symptoms and amelioration of the symptoms after glucose administration [11]. Biochemical findings confirming the diagnosis are the hyperinsulinism and the high levels of peptide C, concomitant with hypoglycemia witnessing the endogenous insulin secretion. After confirming the diagnosis, anatomic localization is necessary. Imaging technologies used to localize the tumor are: Endoscopic abdominal ultrasonography, CT scan or pancreatic MRI. These modalities can identify the exact size and location of an insulinoma, describe its anatomic relationship to surrounding structures and detect the presence of metastatic lesions suggestive of malignancy [12]. Yet, some authors think that preoperative localization of the tumor is not mandatory and that intraoperative localization by experienced surgeons is the most important [13]. In our context, the tumors were detected preoperatively based on abdominal CT scan in three cases out of four.
Treatment relays on surgical excision of the tumor. Surgical procedures depend on the tumor size and its localization. In case of a small and unique tumor that is not encroaching the pancreatic or the bile ducts and in case it was well localized preoperatively and preoperatively, the tumor enucleation is the treatment of choice. In case of a tumor that is invading or in close proximity to the pancreatic duct or major vessels, or suspicious for malignancy with a hard, infiltrating tumor and puckering of the surrounding soft tissue, pancreatic duct dilatation or lymph node involvement, pancreatic resection is indicated [14].
Besides surgery, other techniques have been described with benign insulinomas, such as injection of octreotide, EUS-guided alcohol ablation, Radio Frequency Ablation (RFA), or embolization of an insulinoma of the pancreas [15].
Medical management of insulinoma, used to treat and prevent hypoglycemia, is generally restricted to unresectable metastatic tumors, unsuccessful operation with persistent symptoms, inoperable patients, and patients awaiting or refusing surgery [14].
Conclusion
Insulinomas are rare endocrine tumors that can be life-threatening by causing severe hypoglycemia. Clinical manifestations are diverse and the diagnosis is usually delayed. Biochemical diagnosis is easy, but the preoperative localization of the tumor can be challenging. Surgical resection of the tumor is the treatment of choice and should be done by an experienced surgeon. Risk of reoccurrence is rare after surgery and it usually concerns tumors with high histological grade.
Declarations
Consent: The examination of the patient was carried out in accordance with the principles of the Declaration of Helsinki.
Conflicts of interest: The authors declare no conflict of interest.
References
- Qi Z, Li D, Ma J, Xu P, Hao Y, et al. Insulinoma Presenting as a Complex Partial Seizure: Still a Possible Misleading Factor. Front Neurosci. 2019; 13: 1388.
- Amin S, Kim MK. Islet Cell Tumors of the Pancreas. Gastroenterol Clin North Am. 2016; 45: 83–100.
- Asa SL. Pancreatic endocrine tumors. Mod Pathol. 2011; 24: S66-S77.
- Chatziioannou A, Kehagias D, Mourikis D, Antoniou A, Limouris G, et al. Imaging and localization of pancreatic insulinomas. Clin Imaging. 2001; 25: 275–283.
- Noone TC, Hosey J, Firat Z, Semelka RC. Imaging and localization of islet-cell tumours of the pancreas on CT and MRI. Best Pract Res Clin Endocrinol Metab. 2005; 19: 195–211.
- Kann PH, Rothmund M, Zielke A. Endoscopic ultrasound imaging of insulinomas: Limitations and clinical relevance. Exp Clin Endocrinol Diabetes. 2005; 113: 471–474.
- Gimm O, König E, Thanh PN, Brauckhoff M, Karges W, et al. Intra-operative quick insulin assay to confirm complete resection of insulinomas guided by Selective Arterial Calcium Injection (SACI). Langenbecks Arch Surg. 2007; 392: 679–684.
- Morita S, Machida H, Kuwatsuru R, Saito N, Suzuki K, et al. Preoperative localization of pancreatic insulinoma by super selective arterial stimulation with venous sampling. Abdom Imaging. 2007; 32: 126–128.
- H. B, R. K, A. D, M. B, F. C, W. R, et al. Pancreatic insulinoma: Diagnostic approach and therapeutic modalities. 2006; 113–116.
- Vaidakis D, Karoubalis J, Pappa T, Piaditis G, Zografos GN, et al. Pancreatic insulinoma: Current issues and trends. Hepatobiliary Pancreat Dis Int. 2010; 9: 234–241.
- Rostambeigi N, Thompson GB. What should be done in an operating room when an insulinoma cannot be found? Clin Endocrinol (Oxf). 2009; 70: 512–515.
- Virally ML, Guillausseau PJ. Hypoglycemia in adults. Diabetes Metab. 1999; 25: 477–490.
- Daggett PR, Kurtz AB, Morris DV, Goodburn EA, Le Quesne LP, et al. IS PREOPERATIVE LOCALISATION OF INSULINOMAS NECESSARY? The Lancet. 1981; 317: 483–486.
- Abboud B, Boujaoude J. Occult sporadic insulinoma: Localization and surgical strategy. World J Gastroenterol. 2008; 7; 14: 657–665.
- Rott G, Biggemann M, Pfohl M. Embolization of an insulinoma of the pancreas with trisacryl gelatin microspheres as definitive treatment. Cardiovasc Intervent Radiol. 2008; 31: 659–662.