
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Fertility preservation in growing Teratoma syndrome: Case report
Duna Trobo1*; María Ruiz-Minaya2; Juan Pina1; Beatriz Gutierrez1; Federico Mariano Pérez-Milán1
1Hospital General Universitario Gregorio Marañón, Department of Obstetrics and Gynecology, c/ O’Donnell 48, CP: 28009 Madrid, Spain.
2Hospital 12 de Octubre, Department of Obstetrics and Gynecology, Av de Córdona s/n, CP: 28041 Madrid, Spain.
*Corresponding Author : Duna Trobo
Department of Obstetrics & Gynecology & Reproductive Medicine Hospital, General Universitario Gregorio Marañón. c/ O’Donnell 48, CP: 28009 Madrid, Spain.
Tel: 0034 5290047;
Email: duna.trobo@salud.madrid.org
Received : Jan 03, 2023
Accepted : Feb 08, 2023
Published : Feb 15, 2023
Archived : www.jcimcr.org
Copyright : © Trobo D (2023).
Abstract
Background: Teratomas are the most common ovarian germ cell tumors. Growing teratoma syndrome is a rare condition that entails the appearance of extragonadal teratomas during or after chemotherapy treatment of non-seminomatous germ cell tumors.
Case: We present the case of a 15-year-old patient with recurrent dermoid cysts in the lungs and contralateral ovary after receiving chemotherapy for an immature teratoma in the left ovary. A strategy to preserve fertility was planned.
Conclusion: A fertility evaluation is important due to the high risk of secondary ovarian failure. To the best of our knowledge, this is the first case report describing the different procedures available to preserve fertility in young patients with this syndrome.
Keywords: Immature teratoma; Growing Teratoma syndrome; Fertility preservation; Childhood cancer.
Abbreviations: IOTS: Immature Ovarian Teratomas; GTS: Growing Teratoma; CT Scan: Syndrome Computed Tomography Scan; PET: Positron Emission Tomography; MRI: Magnetic Resonance Imaging AMH: Anti-Müllerian Hormone; BEP: Bleomycin Etoposide, And Cisplatin.
Citation: Trobo D, Ruiz-Minaya M, Pina J, Gutierrez B, Pérez-Milán FM. Fertility preservation in growing Teratoma syndrome: Case report. J Clin Images Med Case Rep. 2023; 4(2): 2288.
Introduction
Ovarian teratomas, also known as dermoid cysts, are the most common ovarian germ cell tumors. Teratomas can be divided into two histological subgroups: Mature and immature teratomas. Immature Ovarian Teratomas (IOTs) are a histological subtype that represent less than 1% of all ovarian cancers [1-3] and account for 10% to 20% of ovarian cancers in women under 20 years of age [3].
Growing Teratoma Syndrome (GTS) is a rare clinical entity that entails the appearance of large intraabdominal or thoracic masses of mature teratoma cells after systemic chemotherapy for the treatment of germinal cell tumors with immature components. We present the case of a 15-year-old patient who had an immature teratoma in the left ovary treated with surgery and chemotherapy and posterior mature teratomas in the lungs and contralateral ovary.
Case report
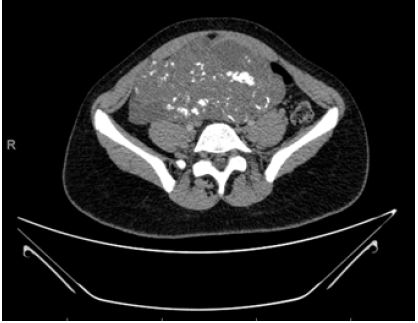
A 15-year-old patient with no personal or family medical history of interest presented to the emergency department complaining of gastrointestinal symptoms with pain in the left iliac fossa and abdominal distension. A CT scan was performed which revealed a solid intraabdominal mass measuring 16 x 16 cm in the left ovary with internal calcifications (Figure 1). Tumor markers, including CA-125, CA 19-9, BhCG and AFP, showed increased levels of AFP, with the rest within normal limits. This patient had menarche three years before when she was 12 years old and her menstrual periods were normal.
An exploratory laparotomy was conducted which found a large mass consisting of solid parts mixed with tumoral cysts of a whitish-yellow color and soft consistency. The tumor was removed completely by means of a left adnexectomy. The histopathological analysis revealed an ovarian mixed germ cell tumor with 90% immature components and 10% vitelline yolk sac tumor. The patient was referred to the fertility unit in order to preserve fertility. At that time, fertility preservation was dismissed due to the malignant histology of the tumor and the need to start chemotherapy urgently.
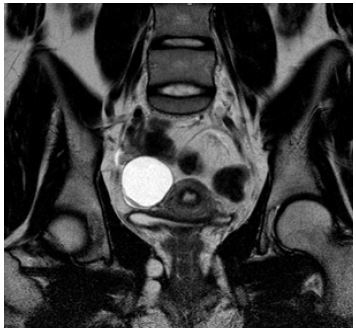
The patient received four cycles of a Bleomycin, Etoposide, and Cisplatin (BEP) chemotherapy regimen. On a PET-CT scan five months after completing treatment, pulmonary nodules were detected. With a suspicion of metastasis, the nodules were removed via a thorascoscopy. Microscopically, the nodules from the left upper lobe were found to be mature teratoma. On a transvaginal ultrasound two months later, a new cyst in the right ovary was observed. The image showed a unilocular cystic mass measuring 24 x 19 mm with a solid papillary mass inside that measured 10 x 9 mm, Doppler score 1, with healthy surrounding ovarian tissue. An MRI test revealed a cystic formation in the right ovary measuring 44 x 33 x 36 mm that contained a solid papillary mass inside. No macroscopic fat component was observed (Figure 2).
The patient was again referred to the fertility unit to plan a fertility preservation strategy due to the risk of losing the right ovary. Even though growing teratoma syndrome was suspected and there was a high probability that this new cyst was also a mature teratoma, it was still possible that it was a metastasis of the original tumor. The patient was in amenorrhea secondary to the chemotherapy received, so conventional stimulation to vitrify oocytes was again ruled out. Pediatric surgeons performed a laparoscopic cystectomy in the right ovary. A gynecologist and a biologist from the fertility unit were present during the surgery in the event the surgeons were unable to perform the cystectomy and a total oophorectomy was needed in order to cryopreserve healthy ovarian tissue. In the end, a cystectomy was possible and the histopathological analysis found it to be a mature teratoma.
Six months after the first surgery, an ovarian reserve study was conducted. An antral follicle count of two in the right ovary and an AMH 0.16 ng/mL were found. At this point, the patient was in amenorrhea and surgery on the right ovarian cyst was pending. Therefore, fertility preservation was postponed.
At present, the patient is well after one year of post-surgical follow-up. No residual tumors have been detected through regular examinations with ultrasounds and scans. The patient regained normal menstrual cycles and another ovarian reserve study found an antral follicle count of nine in the right ovary and an AMH of 1.46 ng/mL.
Given the possibility of a recurrence of ovarian teratomas in the remaining ovarian tissue, the patient was offered the possibility of hormonal stimulation to vitrify oocytes in order to preserve fertility. The patient was informed about the prognosis secondary to the chemotherapy received and the remaining tissue in the right ovary. She accepted the treatment and at present, she is waiting for her period in order to start ovarian stimulation.
Discussion
Benign teratomas are believed to arise from primordial germ cells in the fetus. They are distributed along the lines of migration from the embryonic yolk sac endoderm to other tissues such as the primitive gonads during early embryogenesis. Although these tumors are mainly located in the ovaries, extragonadal tumors can appear anywhere along germ cell migration routes and account for 2% to 5% of all germ cell tumors [4,5]. As they follow migration routes, these tumors typically grow in middle structures like the retroperitoneum, brain, thymus, lungs, liver, and uterus [6].
Growing Teratoma Syndrome (GTS) was first described by Logothetis et al. in 1982. This syndrome leads to the appearance of large masses of metastatic mature teratoma in diverse locations during or after chemotherapy in patients with immature germ cell tumors [7]. The diagnosis of GTS is based on three main criteria: personal history of germ cell tumor, radiological evidence of growing lesions during or after chemotherapy, and normal tumor markers [8]. Surgery is the primary treatment and the outcome depends on the size and location of GTS [9]. Our patient met all the three criteria. A differential diagnosis was made between recurrence of the immature teratoma and GTS. In this case, the main suspicion was GTS, as recurrences of immature teratomas often appear as larger masses with prominent solid components.
Although an ovarian location is infrequent, these patients have a high risk of infertility due to multiple abdominal interventions that reduce the ovarian reserve and the secondary formation of intraabdominal adhesions [10,11]. In our case, the patient had two important risk factors for developing infertility in the future: treatment with gonadotoxic chemotherapy and multiple ovarian surgeries.
The increase in survival rates of young patients with cancer, new reproductive techniques, and a growing interest in quality of life after gonadotoxicity in cancer survivors have highlighted the importance of fertility preservation in young patients [12,13]. Different techniques can be used in order to preserve fertility in oncological patients. The cryopreservation of oocytes and embryos is the standard procedure. However, these procedures require ovarian stimulation for eight to 12 days, which delays the start of oncological treatment. In addition, embryo cryopreservation raises serious ethical dilemmas given that in some oncological patients, the prognosis of the disease is guarded in terms of survival and the technique requires a male partner or the use of sperm from a donor. For this reason, the main technique used is oocyte vitrification. This procedure also requires the patient to have menstrual cycles and most authors consider the upper age limit to be between 35 and 40 years [12]. In prepubertal patients or patients who need to start chemotherapy urgently, cryopreservation of ovarian tissue is the only alternative, but it continues to be an experimental technique [13,14].
In this case, oocyte cryopreservation was the first choice for fertility preservation, but was conditional upon the histological nature of the ovarian tumor. Cryopreservation of ovarian tissue was also a possibility in the event of major difficulty in the surgical approach that would have led to requiring a total adnexectomy instead of a cystectomy.
Conclusion
The appearance of clinical or radiological masses in patients treated with chemotherapy for malignant germ cell tumors should alert clinicians to the possibility of GTS. The early identification and surgical treatment of the syndrome improves the prognosis. Fertility preservation in young patients must be carefully evaluated, as the risk of secondary infertility is high given the exposure to gonadotoxic drugs and multiple gynecological intervention that may lead to a decrease in ovarian reserve.
Declarations
Acknowledgements: The authors would like to thank the Agencia de Traducción Medico-Científica V de A for providing language help.
Conflict of interest: The authors declare no conflict of interests regarding this article.
References
- Talerman A. Germ cell tumors of the ovary. Curr Opin Obstet Gynecol. 1997; 9: 44-47.
- Quirk JT, Natarajan N. Ovarian cancer incidence in the United States, 1992-1999. Gynecol Oncol. 2005; 97: 519–523.
- RCOG. Management of female malignant ovarian germ cell tumours. Scientific Impact Paper Nos. 52, 2016. RCOG Scientific Impact paper No.52; 2016.
- Lim S chul, Kim Y shin, Lee Y han, Lee M sook, Lim J young. Mature teratoma of the uterine cervix with lymphoid hyperplasia. Pathol Int. 2003; 53: 327–331.
- Albany C, Einhorn LH. Extragonadal germ cell tumors: Clinical presentation and management. Curr Opin Oncol. 2013; 25: 261–265.
- Newsom-Davis T, Poulter D, Gray R, Ameen M, Lindsay I, Papanikolaou K, et al. Case report: Malignant teratoma of the uterine corpus. BMC Cancer. 2009; 9: 195.
- Logothetis CJ, Samuels ML, Trindade A, Johnson DE. The growing teratoma syndrome. Cancer. 1982; 50: 1629–1635.
- Abdulraheem EA, Sait MK, Sait KH, Anfinan NM, Elkadi OR. Growing teratoma syndrome with porta hepatis involvement - A case report. Int Med Case Rep J. 2019; 12: 75–78.
- Gorbatiy V, Spiess PE, Pisters LL. The growing teratoma syndrome: Current review of the literature. Indian J Urol IJU J Urol Soc India. 2009; 25: 186–189.
- Shigeta N, Kobayashi E, Sawada K, Ueda Y, Yoshino K, Hori Y, et al. Laparoscopic excisional surgery for growing teratoma syndrome of the ovary: Case report and literature review. J Minim Invasive Gynecol. 2015; 22: 668–674.
- Bentivegna E, Azaïs H, Uzan C, Leary A, Pautier P, Gonthier C, et al. Surgical Outcomes After Debulking Surgery for Intraabdominal Ovarian Growing Teratoma Syndrome: Analysis of 38 Cases. Ann Surg Oncol. 2015; 22: S964-970.
- Del-Pozo-Lérida S, Salvador C, Martínez-Soler F, Tortosa A, Perucho M, et al. Preservation of fertility in patients with cancer (Review). Oncol Rep. 2019; 41: 2607–2614.
- Andersen CY, Kristensen SG, Greve T, Schmidt KT. Cryopreservation of ovarian tissue for fertility preservation in young female oncological patients. Future Oncol Lond Engl. 2012; 8: 595–608.
- von Wolff M, Donnez J, Hovatta O, Keros V, Maltaris T, et al. Cryopreservation and autotransplantation of human ovarian tissue prior to cytotoxic therapy-a technique in its infancy but already successful in fertility preservation. Eur J Cancer Oxf Engl 1990. 2009; 45: 1547–1553.