
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Rhino-orbito-cerebral mucormycosis: A case report and review of the literature
Lin Tuo; Xingxiang Yang*; Renguo Yang*
Department of Infectious Diseases, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, No. 32, 3rd West Section, First Ring Road. Chengdu 600072, China.
*Corresponding Author : Xingxiang Yang &
Renguo Yang
Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, No. 32, 3nd West Section, First Ring Road, Chengdu 600072, China.
Tel: +86-028-83794030;
Email: gg007666@163.com; 719525383@qq.com
Received : Jan 20, 2023
Accepted : Feb 13, 2023
Published : Feb 20, 2023
Archived : www.jcimcr.org
Copyright : © Yang X & Yang R (2023).
Abstract
Background: Mucormycosis is an opportunistic deep-fungal infection requiring urgent intervention. Because of the rapidly and destructively progress, delayed initiation of treatment is associated with increased mortality. We reported the survived case of Rhino-Orbital-Cerebral Mucormycosis (ROCM) after taking liposomal amphotericin B.
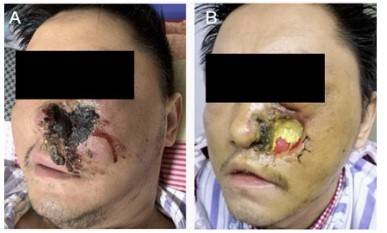
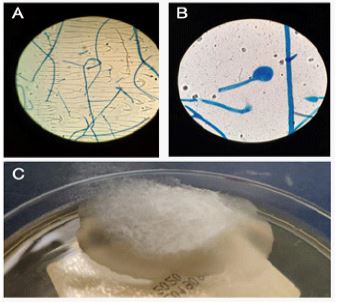
Case presentation: A 43-year-old man with diabetes mellitus type 2 presented fever and general malaise, with nasal congestion, moderate pain in left ocular and left orbitofrontal region radiating to the occipital region. The physical examination revealed facial cellulitis involving his left buccal, black eschars and necrotic ulcers on his left alar of nasal, and white purulent spots on the left palate. Chest CT showed pneumonia progression and associated multiple cavities in both lungs (the maximum diameter was about 45 mm), and patchy shadows in the right lung. Fortunately, the presence of broad (at least 6-16 um wide), non-septate or pauci-septate hyphae with wide-angle branching were seen in secretion from affected tissue using direct microscopy. Furthermore, the cottony white colony were appeared after the secretion cultured in 37.0. Based on the clinical presentation, culture results and microscopic examination, a diagnosis of Rhino-orbital-cerebral mucormycosis was made. Furthermore, after three weeks of antifungal (intravenous liposomal amphotericin Band oral posaconazole), antimicrobial therapy and facial debridement, the patient had improved general condition and was discharged.
Conclusions: We analysis one case of recently diagnosed and treated ROCM, and reviews 28 confirmed cases of ROCM in the English literature, aiming to provide a reference for the diagnosis and treatment of ROCM. It is necessary to be alert to the occurrence of ROCM in immuno compromised patients. Furthermore, the related symptoms of ROCM that have occurred should be early identified, diagnosed and treated.
Keywords: Rhino-Orbito-Cerebral Mucormycosis (ROCM); Infection disease; Fungal infection.
Citation: Tuo L, Yang X, Yang R. Rhino-orbito-cerebral mucormycosis: A case report and review of the literature. J Clin Images Med Case Rep. 2023; 4(2): 2293.
Introduction
Mucormycosis is a rare disease with high mortality, which describes infections caused by an opportunistic deep fungal of the order Mucorales [1]. After Aspergillus, Mucorales fungi is the second commonest pathogen in immunocompromised patients with haematopoietic stem cell transplantation, solid organ transplantation or haematological malignancy [2]. In addition, mucormycosis in immunocompetent patients is often accompanied by diabetes mellitus, trauma or iatrogenic injury. Rhino-Orbital-Cerebral Mucormycosis (ROCM) was the most frequently reported type, followed by cutaneous, pulmonary and disseminate mucormycosis. ROCM can spread contiguously into nasal cavity, maxilla, paranasal sinuses and orbit through the junction of skin and mucosa, and finally causes intracranial infection due to cascular invasion or bone destruction [3,4]. ROCM requires urgent intervention because of the rapidly progressive infection and poorly prognosis. However, non-specific clinical manifestation and incorrect morphological diagnosis often lead to misdiagnosis, delayed initiation of therapy and increased mortality of Mucor mycosis. This paper reports one case of recently diagnosed and treated ROCM, and reviews 28 confirmed cases of ROCM in the English literature, aiming to provide a reference for the diagnosis and treatment of ROCM.
Case report
A 43-year-old man with type 2 diabetes mellitus diagnosed in the previous 4 years, treated with metformin (200 mg/day) and had poor treatment compliance. Fasting plasma glucose was 8-10 mmol/L and 2-Hour postprandial blood glucose was 11-16 mmol/L in the recent 10 days. He presented in the emergency department of other hospital complaining of nasal congestion bloody snot and left facial swelling. He was diagnosed as acute bacterial nasal/sinus infection, with antibiotic prescription (vancomycin and meropenem). Four days later he comes to our department with low fever and general malaise, with nasal congestion, moderate pain in left ocular and left orbitofrontal region radiating to the occipital region.
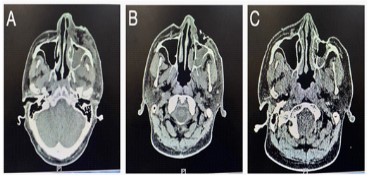
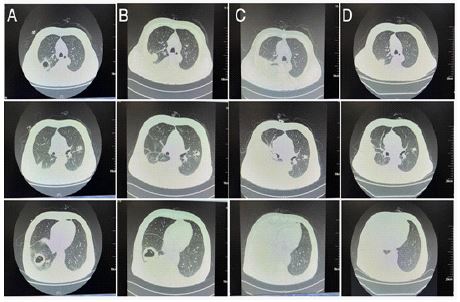
At the admission, the patient was fully conscious and vital stable with a temperature 36.5, a blood pressure 108/71 mmHg and a pulse rate of 78 beats/min. He had uncontrolled diabetes mellitus with diabetic ketoacidosis. The physical examination revealed facial cellulitis involving his left buccal, black eschars and necrotic ulcers on his left alar of nasal, and white purulent spotson the left palate (Figure 1, tRoutine blood tests indicated elevation of glycated haemoglobin (13.3%), procalcitonin (0.37 ng/ml) , leukocytosis (16.78 × 109/L), percentage of neutrophils (80.6%) and random blood glucose (16.8 mmol/L). A facial Computed Tomography (CT) scan was performed and revealed irregular swelling on the left side of face and maxillary sinus, left ethmoid sinusitis, maxillary sinusitis and sphenoid sinusitis (Figure 2). A chest Computed Tomography (CT) scan showed high-density nodular shadow with a diameter of 20 mm in the upper lobe of the right lung and multi-density mass shadow with a diameter of 30 mm in the lower lobe of the right lung (Figure 3). The first clinical diagnosis indicated acute nasal/facial infection and pneumonia, and therefore antibiotics (meropenem 500 mg q6 h and vancomycin 500 mg q6 h) were performed.
However, on the third day of admission, despite being good glycemic control and continuous debridement, the patient continued to be feverish (37.6) with dizziness, cough and expectoration. Repeated chest CT result showed pneumonia progression, and associated multiple cavities in both lungs (the maximum diameter was about 45 mm), and patchy shadows in the right lung (Figure 3). Considering the poor effect of anti-infection treatment, the etiological basis was vital. Fortunately, the presence of broad (at least 6-16 um wide), non-septate or pauci-septate hyphae with wide-angle branching were seen in secretion from affected tissue using direct microscopy. Furthermore, the cottony white colony were appeared after the secretion cultured in 37.0 (Figure 4). Based on the culture results and microscopic examination, a provisional diagnosis of a Mucorales fungi infection was made. What’s more, clinical and radiographic data were suggestive of early presentation of rhino-orbito-cerebral mucormycosis and pulmonary mucormycosis. Anti-bacterial (meropenem and vancomycin) were suspended due the unfavorable disease progression with the initial treatment. The recommended starting treatment of ROCM were intravenous liposomal amphotericin B (70 mg/day) and oral posaconazole (400 mg bid). During the treatment, the repeated chest CT results showed that decreased patchy shadows, unchanged multiple cavities in both lungs, and new-occurred pleural effusion. Considering the possibility of bacterial co-infection, we added piperacillin tazobactam (4.5 g q8h). After three weeks of antifungal, antimicrobial therapy and facial debridement, the patient had improved general condition and was discharged. After that, the patient took oral Posaconazole at home for a long time, and further underwent facial plastic surgery 4 months later. The postoperative clinical profile picture of the patient at nine months showing resolution of facial swelling and formation of hyperplasia tissue near the left buccal and left alar of nasal (Figure 5).

Discussion
Literature analysis of Rhino-orbito-cerebral Mucormycosis
20 case reports with complete data of ROCM from 2011 to 2021 were retrieved from Pubmed, which in total reported 28 cases [5-23].
Clinical features of ROCM
Among the 28 ROCM patients identified, the youngest was 4 years old, while the oldest was 87 years old. Most were male with diabetes. It is mainly acute onset, the course of the disease range from several days to several months, and the average onset time is 45 days. Most patients have multiple complications, such as prostate cancer, acoustic neuroma, B-cell lymphoma, alcohol abuse, cirrhosis and hypertension, especially diabetes. More than half of the patients have a history of type 1 diabetes, which insulin-controlling is not effective.
The symptoms are also diverse. Among these patients, 53.6% had fever, 71.4% had local pain, such as oral cavity, nasal root, cheek and so on, and 75% had elevated leukocytes or neutrophils, as indicated in Table 1. A series of symptoms were caused by vascular embolism and tissue necrosis in different tissues, which caused nasal congestion, runny nose, fever and headache by involving nasal sinuses. Furthermore, the affected tissue finally form necrotic black eschar. In addition, 28.6% of patients had pulmonary infection, pleural effusion and so on, which may be caused by fungal infection of ROCM.
Table 1: Basic information about the ROCM patient n (%).
| Age (yr) | 47.5 ± 21.4 |
|---|---|
| Gender (male / female) | 14/14 |
| Healthy | 3 (0.11) |
| Diabetics | 15 (0.56) |
| Cancer | 3 (0.11) |
| Fever | 15 (0.56) |
| Headache | 20 (0.71) |
| Loss of vision | 4 (0.14) |
| Swollen eyelid | 19 (0.68) |
| Gastrointestinal symptoms | 2 (0.07) |
Imaging feature of ROCM: The typical clinical manifestation of ROCM is the rupture of facial and maxillofacial defects, mostly accompanied by the attachment of white pseudomembrane. Some appear in the mouth, some appear in the eyes or the maxilla. The characteristic imaging data are mainly manifested in the cavity and nodule shadow of chest CT. Voids and nodules appeared in 10.7% of patients. However, there are still 5 (17.9%) patients with atypical lung changes, such as increased density, which is difficult to distinguish from pulmonary bacterial infection.
Diagnosis of ROCM
Mucormycosis is a fatal fungal infection caused by mucormycosis. In addition to aspergillosis and candidiasis, mucormycosis is the third invasive fungal infection. Rhizopus, Mucor and Listeria are common pathogens causing mucormycosis. Patients with immune deficiency are infected by Mucor spores inhaled into the air. They can also be infected through skin, food, intravenous infusion, mosquito bites and so on. Mucormycosis can be divided into nose eye brain type, lung type, skin type, gastrointestinal type, widely disseminated type and mixed infection type according to the infection site, and its mortality fluctuates in 40-80% according to the infection site.
The diagnosis of ROCM depends on the clinical manifestation, as indicated in Table 2, making it easily misdiagnosed as other fungal infections. The examination of pathogenic microorganisms is very important. These are no standardized method for serological detection of Mucor specific antigen, and fungal culture and biopsy are the gold standard for the diagnosis of mucormycosis. None of the 28 patients was diagnosed only by clinical manifestations. About 17 (60.7%) patients were diagnosed by microbial microscopy, which showed less branches and obtuse tentacles under microscopic examination. Only 3 (10.7%) patients were diagnosed by culturing related pathogenic microorganisms, and there may be diagnosed by next generation sequencing.
Table 2: Diagnosis and treatment about the ROCM patient n (Total 28) (%).
| Diagnostic methods | |
| Microbial cultivation | 3 (0.11) |
| Microscopic examination | 17 (0.61) |
| Next generation sequencing | (0.07) |
| Treatment | |
| Surgeon | 11 (0.39) |
| Antifungal drug | 3 (0.8) |
| Liposomal amphotericin B | 18 (0.64) |
| Posaconazole | 4 (0.14) |
| Piperacillin/tazobactam | 1 (0.04) |
| Outcome | |
| Survival | 18 (0.64) |
| Died | 9 (0.3) |
| Unknown | 1 (0.04) |
Treatment of ROCM
The treatment of ROCM mainly involves three aspects. Firstly, we should strengthen wound drainage and disinfection. Secondly, the underlying diseases such as diabetes should be well-controlled. On the end, it is important for anti-infective treatment. The main treatments of anti-infection used in 28 patients were liposomal amphotericin B (64.3%) and posaconazole (14.3%).The outcome of the disease mainly depends on the effect of anti-infective treatment and the patients’ underlying disease. The mortality of ROCM was about 32.1%. Overall, the treatment for Mucormycosis depends on the basic situation and invasion site of the patient, which generally treated for several weeks to months or even years until the symptoms disappeared and the imagine improved.
Conclusion
Mucormycosis is an opportunistic deep-fungal infection requiring urgent intervention. Its form of pathogenic was confirmed in 1815 [24]. The first case of Mucormycosis in humans was described in 1855 [25], and the first recorded case of chronic infection was described in 1964 [26]. Because of the rapidly and destructively progress, delayed initiation of treatment is associated with increased mortality. Maximizing the survival rate requires rapid diagnosis and early intervention, including the immediate participation of multidisciplinary medical, surgical, imaging and laboratory teams. The patients in our study were survived, which is also related to the rapid diagnosis and treatment through the multi-disciplinary cooperation. In conclusion, it is necessary to be alert to the occurrence of ROCM in immunocompromised patients. Furthermore, the related symptoms of ROCM that have occurred should be early identified, diagnosed and treated.
Declarations
Conflict of interest: None to declare.
Author contributions: TL and YRG reviewed the literature and contributed to manuscript drafting; YXX performed microscopic examination and contributed to manuscript drafting. All authors read and approved the final manuscript.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethics approval and consent to participate: Not required by the relevant ethics committee. The patient signed an informed consent form for the treatment provided.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consentis available for review by the Editor-in-Chief of this journal.
Financial support and sponsorship: The authors of this study declare no sources of funding for this study.
Competing interests: The authors declare that they have no competing interests.
References
- Skiada A, Lass-Floerl C, Klimko N, Ibrahim A, Roilides E, Petrikkos G, et al. Challenges in the diagnosis and treatment of mucormycosis. Med Mycol. 2018; 56: 93–101. https://doi.org/10.1093/mmy/myx101
- Pilmis B, Alanio A, Lortholary O, Lanternier F, et al. Recent advances in the understanding and management of mucormycosis. F1000 Research. 2018; 7: F1000. Faculty Rev-1429. https://doi.org/10.12688/f1000research.15081.1
- Hassan MIA, Voigt K. Pathogenicity patterns of mucormycosis: Epidemiology, interaction with immune cells and virulence factors. Med Mycol. 2019; 57: S245–S256. https://doi.org/10.1093/mmy/myz011
- Agrawal R, Yeldandi A, Savas H, Parekh ND, Lombardi PJ, Hart EM, et al. Pulmonary Mucormycosis: Risk Factors, Radiologic Findings, and Pathologic Correlation. Radiogr Rev Publ Radiol Soc N Am Inc. 2020; 40: 656–666. https://doi.org/10.1148/rg.2020190156
- Martel J, Anders U, Taylor E, Martel J, et al. Acute orbital apex syndrome and rhino-orbito-cerebral mucormycosis. Int Med Case Rep J. 2015; 93. https://doi.org/10.2147/IMCRJ.S83036
- Kou C, Rendo M, Kline D, Bishop B, Yun HC, et al. An unusual cause of bowel obstruction: Rhizopus Arrhizus diverticulitis. Med Mycol Case Rep. 2019; 25: 15–18. https://doi.org/10.1016/j.mmcr.2019.06.004.
- Wolkow N, Jakobiec FA, Stagner AM, Cunnane ME, Piantadosi AL, et al. Chronic orbital and calvarial fungal infection with Apophysomyces variabilis in an immunocompetent patient. Surv Ophthalmo. 2017; 62: 70–82. https://doi.org/10.1016/j.survophthal.2016.05.006
- Gutiérrez Delgado EM, Treviño González JL, Montemayor Alatorre A, Ceceñas Falcón LA, Ruiz Holguín E, et al. Chronic rhino-orbito-cerebral mucormycosis: A case report and review of the literature. Ann Med Surg. 2016; 6: 87–91. https://doi.org/10.1016/j.amsu.2016.02.003
- Salehi MR, Shahi F, Rizvi FS, Ghaderkhani S, Zainaldain H, et al. Combination antifungal therapy without craniotomy in an immunocompromised patient with rhino-orbito-cerebral mucormycosis: A case report. Casp J Intern Med. 2020; 11: https://doi.org/10.22088/cjim.11.2.227.
- Angali R, Jeshtadi A, Namala V, Gannepalli A. Fatal rhino-orbito-cerebral mucormycosis in a healthy individual. J Oral Maxillofac Pathol. 2014; 18: 460. https://doi.org/10.4103/0973-029X.151355
- Chaudhry A, Hirano SA, Hayes TJ, Torosky C. Fatal rhino-orbito-cerebral mucormycosis in a patient with liver disease. J Am Acad Dermatol. 2011; 65: 241–243. https://doi.org/10.1016/j.jaad.2010.01.002
- Beiglboeck FM, Theofilou NE, Fuchs MD, Wiesli MG, Leiggener C, et al. Managing mucormycosis in diabetic patients: A case report with critical review of the literature. Oral Dis odi. 2021; 13802. https://doi.org/10.1111/odi.13802
- Irtan S, Lamerain M, Lesage F, Verkarre V, Bougnoux ME, et al. Mucormycosis as a rare cause of severe gastrointestinal bleeding after multivisceral transplantation. Transpl Infect Dis. 2013; 15: E235–E238. https://doi.org/10.1111/tid.12147
- R R, MR M, Kumar SP. Mucormycosis Following Tooth Extraction in a Diabetic Patient: A Case Report. Cureus. 2020; https://doi.org/10.7759/cureus.9757
- Bae MS, Kim EJ, Lee KM, Choi WS. Rapidly Progressive Rhino-orbito-cerebral Mucormycosis Complicated with Unilateral Internal Carotid Artery Occlusion: A Case Report. Neurointervention. 2012; 7: 45. https://doi.org/10.5469/neuroint.2012.7.1.45
- Chen Y, He Y, Zhou H, Wang M, Su S, et al. Rapidly progressive rhino-orbito-cerebral mucormycosis in a patient with type 2 diabetes: A case report. Exp Ther Med. 2017; 3.
- Manjunath KS, Shivaswamy S, Kulkarni JD, Venkatachalaiah RK, et al. Rhino-Orbito-Cerebral Mucormycosis (ROCM) with internal carotid artery stenosis in a diabetic patient with caries tooth and oroantral fistula. Case Rep. 6.
- Navarro Perea C, Cañas Zamarra I, Mencía Gutiérrez E, Revilla Sánchez E, Lago Llinás MD, et al. Bengoa-González Á Rhino-Orbito-Cerebral Mucormycosis: Two Cases with Amaurosis as Presentation, Medical Surgical Management and Follow-Up. Case Rep Ophthalmol Med. 7.
- Raffa LH Rhino–orbito–cerebral mucormycosis following penetrating keratoplasty. 4.
- Erami M Rhinocerebral mucormycosis due to Rhizopus oryzae in a diabetic patient: A case report. 7
- Irugu DVK, Gupta M, Sharma P, Ramteke PPS, Sharma SC, et al. Temporal Bone Osteomyelitis in a Child Closely Resembles Lateral Sinus Thrombosis: A Case Report. 2018; 5.
- Narayanan S, Panarkandy G, Subramaniam G, Radhakrishnan C, Thulaseedharan N, et al. The “black evil” affecting patients with diabetes: A case of rhino orbito cerebral mucormycosis causing Garcin syndrome. Infect Drug Resist. 6.
- Ac K. Visual Outcome With A Multimodality Approach In A Case Of Rhinoorbito- Cerebral Mucormycosis. 2016; 6: 8.
- Handa KK, Handa A, Panda N, Mann SBS, et al. Primary chronic mucormycosis. Indian J Otolaryngol Head Neck Surg. 1996; 48: 232–234. https://doi.org/10.1007/BF03048618
- Finn DG, Farmer JC. Chronic mucormycosis. The Laryngoscope. 1982; 92: 761–766. https://doi.org/10.1288/00005537-198207000-00009
- Harrill WC, Stewart MG, Lee AG, Cernoch P, et al. Chronic rhinocerebral mucormycosis. The Laryngoscope. 1996; 106: 1292–1297. https://doi.org/10.1097/00005537-199610000-00024.