
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Disseminated tuberculosis presenting as venous thromboembolism
*Corresponding Author : Ujjawal K Shriwastav
Virbhadra Road, AIIMS Rishikesh, Uttarakhand, India.
Tel: 08521260393;
Email: drujjawalshriwastav@gmail.com,
drujjawalshriwastav@gmail.com.
Received : Jan 25, 2023
Accepted : Feb 13, 2023
Published : Feb 20, 2023
Archived : www.jcimcr.org
Copyright : © Shriwastav UK (2023).
Abstract
Tuberculosis is one of the leading causes of morbidity and mortality throughout the world which can have both pulmonary and extrapulmonary manifestations. Among the myriad extra pulmonary manifestations of tuberculosis, Deep Vein Thrombosis is rare. We present a case of middle-aged lady who presented with progressive painful swelling of the left upper limb associated with intermittent low-grade fever spikes. Upon evaluation she was found to have deep venous thrombosis, along with subsegmental pulmonary embolism on her initial evaluation. Further workup of the patient revealed bilateral pleural effusion and constrictive pericarditis along with microbiological evidence of Mycobacterium tuberculosis. The patient was started on anti-tubercular therapy along with therapeutic anti-coagulation after which there was a substantial clinical improvement. Though rare, this case elucidates venous thrombosis risk associated with one of the most common diseases in developing countries.
Keywords: Tuberculosis; Virchow’s triad; Venous thromboembolis; Pulmonary embolism.
Citation: Shriwastav UK. Disseminated tuberculosis presenting as venous thromboembolism. J Clin Images Med Case Rep. 2023; 4(2): 2294.
Introduction
Tuberculosis is the 13th leading cause of death worldwide and second major infectious killer after COVID-19 with an incidence of 10.6 million people in the year 2021 [1]. It has been the main culprit leading to significant morbidity and mortality in developing countries like India. Despite being rare, active or disseminated tuberculosis has been suggested to be an emerging risk factor for deep vein thrombosis with prevalence of around 1.5-3.4% as found in several studies [2]. Tuberculosis has been shown to affect all three domains [hypercoagulability, endothelial injury and stasis] of Virchow’s triad explained in the pathogenesis of VTE.
Case presentation
A 25-year-old lady without any known addictions and comorbidities presented to a tertiary care center with insidious onset, painful, progressive swelling of left upper limb for two weeks associated with intermittent spikes of low-grade fever spikes during the evening hours. The swelling was not associated with any history of trauma, immobilization or cannulation/instrumentation in recent or past. Detailed history revealed that patient had been having intermittent low grade evening rise of temperature associated with periods of non-productive cough for six months which subsided with over-the-counter anti-pyrectics and cough suppressants respectively but without substantial improvement. There was no history of shortness of breath, chest pain, jaundice, decreased urine output, froth in urine, joint pain or recurrent abortions in the past. She lived in a joint family, had an uneventful childbirth one year back and gave no history of oral contraceptive intake. However, there is a history of contact with a case of active tuberculosis under anti-tubercular therapy in the family.
On examination, she was febrile, pale and thin built but hemodynamically stable. Left upper limb was swollen and tender with limited range of active motion without any redness or pus discharge. Peripheral pulses were present. General physical examination did not reveal any obvious or significant lymphadenopathy and her breast examination were within normal limits. On auscultation of chest, there was decreased breath sounds in bilateral basal regions.
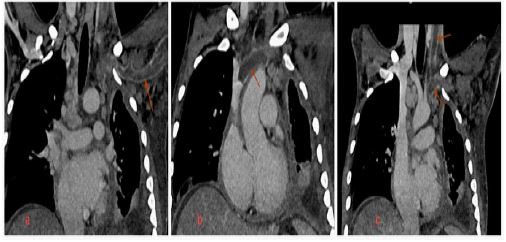
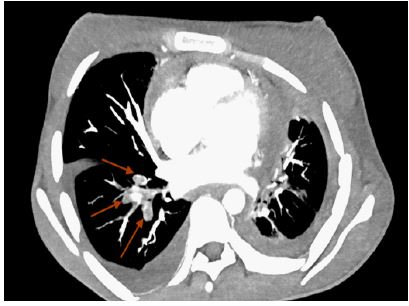
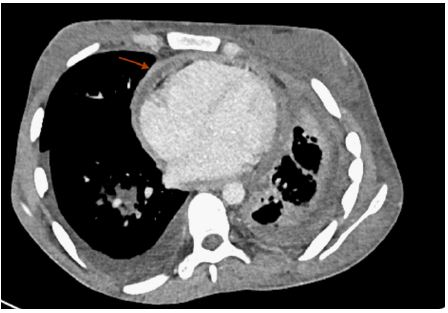
On further evaluation, hemogram showed moderate anemia. Color Doppler scan of left upper limb showed echogenic thrombus within left internal jugular vein, subclavian and axillary vein completely occluding the lumen without any color flow or compressibility. The right upper limb and bilateral lower limb color Doppler scan was negative for any thrombus. Thrombophilia workup was negative with normal Protein C, Protein S and Anti-thrombin III levels. ANA and APLA profile were also negative for the patient. 2D-echocardiography showed right ventricular dysfunction along with features of constrictive pericarditis. A CT-Pulmonary angiography was obtained which showed thromboembolism of subsegmental branches of right lower pulmonary artery along with minimal left pleural effusion. Noticeable and significant mediastinal lymphadenopathy was also seen (Figures 1,2,3).
Ultrasound guided diagnostic pleural effusion tapping was done which was exudative, along with positive for acid-fast bacilli in Modified Ziehl–Neelsenstaining. Rifampicin sensitive Mycobacterium tuberculosis was detected on Cartridge Based Nucleic Acid Amplification Test (CB-NAAT). The patient was initiated on anti-coagulation and weight based Anti-Tubercular Therapy (ATT). Subsequently, there was gradual resolution in swelling and fever spikes. Patient was later discharged on anti-tubercular therapy along with Dabigatran.
Discussion
Disseminated tuberculosis is defined as involvement of two or more non-contagious sites/organ systems due to lympho-hematogenous spread of Mycobacterium tuberculosis. Epidemiological data has suggested that one-fourth or more case of tuberculosis are extra-pulmonary out of which less than almost 20% cases are disseminated tuberculosis [3]. The exact mechanism of disseminated of mycobacterium tuberculosis is not clear but it has been suggested that the erosion of epithelial cells of alveoli leads to entry to bacteria into pulmonary veins resulting into dissemination [4].
The study of various reports on common clinical manifestation and organ system involvement in a case of disseminated tuberculosis suggests that constitution clinical features, lymphadenopathy, pleural effusion and ascites tops the list among various others manifestations [5]. The review of literature from the past has expounded active tuberculosis to be one of the emerging risk factors for development of Deep vein thrombosis with a prevalence of around 1.5-3.4% [2].
The prevalence of venous thromboembolism in form of DVT and Pulmonary embolism is underestimated as they are often silent despite being common. The pathogenesis of venous thrombosis is explained by Virchow’s triad consisting triad of hypercoagulability, venous stasis and endothelial injury [6]. Among numerous risk factors which has been explained for the development of venous thrombosis, infectionis one of them. Sepsis is an example of systemic inflammation with organ dysfunction where disseminated intravascular coagulation has been observed as a major complication and cause of death. The coagulation activation and immunothrombosis has been considered hallmarks of sepsis [7].
Apart from sepsis and hospital settings, similar association between infection and thrombus formation can be found in community setting [8]. One of the examples of community acquired infection is tuberculosis, which is caused by acid fast bacilli Mycobacterium tuberculosis. There have been several mechanisms to explain venous thrombo-embolism in tuberculosis like induction of inflammation, transient hypercoagulable state and direct endothelial injury. Tuberculosis is an pro-inflammatory state which has been associated with increase in acute phase reactants like elevated plasma fibrinogen, which when coupled with decrease in anti-thrombin III appears to support the development of DVT in TB [9]. Thus, Tuberculosis has been described as being one of the hypercoagulable state with enhanced activation of coagulation along with altered mechanisms of anti-coagulation [10]. There has been report to suggest that tuberculosis can result into development of anti-phospholipid antibodies ensuing thrombosis of vessels [11]. Another widely accepted mechanism for the development of venous thrombosis in active tuberculosis has been put forward on account to the use of Rifampicin in the first line treatment of TB [12]. Our case has been a classical example of community acquired infection related thrombosis of large veins. After ruling out all the other causes of thrombosis in a young female, we concluded that disseminated tuberculosis lead to DVT in this case.
Conclusion
Among myriad clinical manifestations of disseminated tuberculosis, deep venous thrombosis and pulmonary embolism could be the presenting manifestations. Despite the prevalence being very low, there have been many case reports explaining the induced coagulation and suppressed anti-coagulation resulting in VTE in cases of active tuberculosis. Early identification and anticipation of such complications with timely initiation of treatment, especially in resource poor settings, can result in a significant decrease in mortality and morbidity associated with it.
References
- Tuberculosis [TB] [Internet]. [cited 2022 Dec 19]. Available from: https://www.who.int/news-room/fact-sheets/detail/tuberculosis
- Gupta A, Mrigpuri P, Faye A, Bandyopadhyay D, Singla R, et al.Pulmonary tuberculosis - An emerging risk factor for venous thromboembolism: A case series and review of literature. Lung India. 2017; 34: 65–69.
- Sharma SK, Mohan A, Sharma A. Miliary tuberculosis: A new look at an old foe. J Clin Tuberc Other Mycobact Dis. 2016; 3: 13–27.
- The mechanisms and consequences of the extra-pulmonary dissemination of Mycobacterium tuberculosis – Science Direct [Internet]. [cited 2022 Dec 21]. https://www.sciencedirect.com/science/article/abs/pii/S1472979210000880?via%3Dihub
- Khan FY. Review of literature on disseminated tuberculosis with emphasis on the focused diagnostic workup. J Family Community Med. 2019; 26: 83–91.
- Bagot CN, Arya R. Virchow and his triad: a question of attribution. Br J Haematol. 2008; 143: 180–190.
- Tani VM, Assis-Mendonça GR, Silva TB da, Rogerio F, Paula EVD, et al. Microvascular thrombosis in sepsis: An autopsy study. Thrombosis Research. 2017; 156: 23–25.
- Smeeth L, Cook C, Thomas S, Hall AJ, Hubbard R, Vallance P, et al. Risk of deep vein thrombosis and pulmonary embolism after acute infection in a community setting. The Lancet. 2006; 367: 1075–1079.
- Robson SC, White NW, Aronson I, Woollgar R, Goodman H, Jacobs P, et al. Acute-phase response and the hypercoagulable state in pulmonary tuberculosis. Br J Haematol. 1996; 93: 943–949. https://doi.org/10.1046/j.1365-2141.1996.d01-1722.x
- Kager LM, Blok DC, Lede IO, Rahman W, Afroz R, et al. Pulmonary tuberculosis induces a systemic hypercoagulable state. J Infect. 2015; 70: 324–334. https://doi.org/10.1016/j.jinf.2014.10.006
- Suárez Ortega S, Artiles Vizcaíno J, Balda Aguirre I, Melado Sánchez P, et al. A tuberculosis como factor de riesgo de trombosisvenosa [Tuberculosis as risk factor for venous thrombosis]. An Med Interna. 1993; 10: 398-400. Spanish. https://europepmc.org/article/med/8218787
- White NW. Venous thrombosis and rifampicin. Lancet. 1989; 2: 434–435.