
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Hemorrhagic stroke in the context of pre-eclampsia on
pregnancy of 28 weeks of gestation: A case report and
review of the literature
Abraham Alexis Sanoh; Alpha Boubacar Conte*; Sofia Jayi; Fatima Zohra Fdili Alaoui; Hikmat Chaara; Moulay Abdelilah Melhouf
Department of Obstetrics and Gynecology 2, University Hospital of Fez, Sidi Mohamed Ben Abdellah University of Fez, Morocco.
*Corresponding Author : Alpha Boubacar Conte
Resident, Department of Obstetrics and Gynecology 2, Hassan II University Hospital of Fez, Morocco.
Email: abcconte33@yahoo.com
Received : Jan 30, 2023
Accepted : Feb 14, 2023
Published : Feb 21, 2023
Archived : www.jcimcr.org
Copyright : © Conte AB (2023).
Abstract
Strokes are rare but serious accidents during pregnancy, they are responsible for high mortality and morbidity, preeclampsia and stroke are significantly linked. Endothelial dysfunction, impaired cerebral self-regulation, and severe high blood pressure are, probably, the cause of many strokes in pregnant women. We report a case of brainstem hemorrhagic stroke in a 28-year-old patient admitted for the management of severe preeclampsia in a pregnancy of 28 weeks of gestation complicated by anemiaand hemorrhagic stroke discovered during the hospitalization. Through this case, we did a brief review of the literature.
Keywords: Pre-eclampsia; Hemorrhagic stroke; Brainstem.
Citation: Sanoh AA, Conte AB, Jayi S, Alaoui FZF, Chaara H, et al. Hemorrhagic stroke in the context of pre-eclampsia on pregnancy of 28 weeks of gestation: A case report and review of the literature. J Clin Images Med Case Rep. 2023; 4(2): 2296.
Introduction
Pre-eclampsia is a specifically obstetrical pathology, whose prevalence is estimated between 1 to 2% of pregnant women and which can, in its severe forms, be life-threatening for the mother and the unborn child [1]. In France, maternal mortality secondary to hypertensive gravidic pathologies decreased by 50% in 10 years, reaching a ratio of 0.5/100,000 live births in 2010 - 2012 according to a report of the confidential national survey on maternal deaths [2]. Although it is not the leading cause of maternal mortality in France, severe pre-eclampsia remains one of its main causes. Pre-eclampsia is also responsible for a third of premature births in France [3], in Morocco it is estimated between 0.61% and 6.65% of cases especially in young primiparous (more than 60% aged less than 30 years and more than 50% of primiparous women).
Pre-eclampsia is defined as the appearance of high blood pressure (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg) associated with proteinuria (≥300 mg/24 H) or without proteinuria but with the presence of acute pulmonary edema and / or acute renal failure and / or hepatic cytolysis and / or thrombocytopenia, after 20 weeks of gestation [3]. The association between preeclampsia and cerebral hemorrhage has been recognized since 1881 [4], Stroke is responsible for 50% of deaths in preeclamptic patients [4]. We report the observation of a patient who had preeclampsia + anemia at 5 g/l complicated by cerebrovascular hemorrhagic accident.
Through this case, we submit a review of the literature reporting the particularities of this exceptional complication of preeclampsia to ensure rapid and adequate care of patients.
Case presentation
F.D, 28-year-old patient, G4P2 with a history of preeclampsia during the previous pregnancy, who consults for high blood pressure figuress at 16/11 mmHg with a positive urine strip with two crosses + anemic syndrome on pregnancy not followed by 28 weeks of amenorrhea.
The examination found a conscious patient 15/15 Glasgow score, asthenic, conjunctive discolored with puffiness of the face associated with headache-tinnitus - phosphenes The obstetric examination had found a uterine height 22 cm lower than gestational age, fetal heart sounds perceived at 145 beats per minute without uterine contraction.
Faced with this clinical picture, she benefited from an antihypertensive treatment based on 1 cc of nicardipine 10 mg and Aldomet 500 mg and a loading dose of magnesium sulfate supplemented by a biological assessment finding anemia with an Hb level of 5.5 microcytic hypochrome, a platelet count of 190000, a correct hemostasis assessment, correct liver function with moderate acute renal failure.
The patient was hospitalized for adequate management and monitoring of severe preeclampsia. During monitoring, the patient presented prostration without tonic-clonic seizures, hence her immediate transfer to intensive care where the examination found a disoriented, hemodynamically stable patient, blood count showed Hb 6.6, platelets 119000, no hepatic cytolysis, LDH 500, Haptoglobin 0.43, D-Dimer 4070 with worsening renal function.
The patient was hospitalized for adequate management and monitoring of severe preeclampsia. During monitoring, the patient presented prostration without tonic-clonic seizures, hence her immediate transfer to intensive care where the examination found a disoriented, hemodynamically stable patient, blood count showed Hb 6.6, platelets 119000, no hepatic cytolysis, LDH 500, Haptoglobin 0.43, D-Dimer 4070 with worsening renal function.
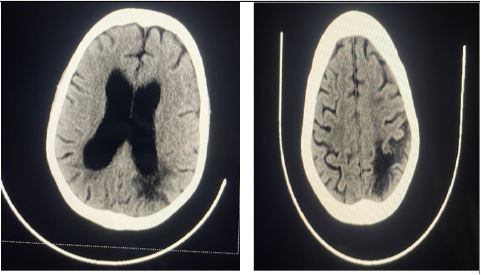
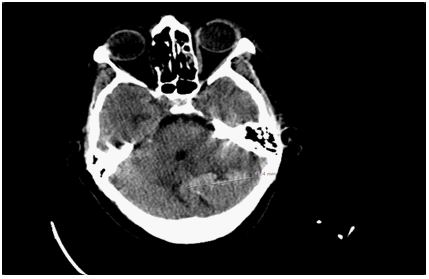
24 hours after his admission and in front of the delay in awakening, a brain scan was performed and highlighted the presence of hypodense corticosteroid range under cortical mainly subcortical asymmetric bilateral occipito at the left occipito level and right parietal not systematized associated with a left cerebellar intraparenchymal hemorrhage with triventricular hydrocephalus. This CT scan was supplemented by a cerebral MRI which highlighted the presence of corticosteroid range under cortical mainly subcortical bilateral asymmetrical at the level left occipito parietal and right parietal not systematized to an arterial territory in hypo signal T1, hypersignal T2 and FLAIR not restrictive in diffusion; presence of petechiae of the white matter subcortical sus tentorial at the level of the semioval center and corona radiata presenting the mèmy characteristics as the above described beaches; presence of bilateral cerebellar intraparenchymal beaches more marked on the left described in hyposignal T1, T2, FLAIR surrounded by a peripheral edge in hypersignal T1 non-restrictive diffusion surrounded by a FLAIR hypersignal related to perilesional edema which together is responsible for a mass effect on the vermis which is compressed. Triventricular dilation with the junctions of the 2 lateral ventricles measured at 24 mm on the right and 17 mm on the left and V3 measured at 10 mm. It is associated with a discrete hypersignal T2 under ependymal in relation to trans ependymal resorption all in favor of a PRES complicated syndrome of cerebellar hemorrhagic rearrangements and active triventricular hydrocephalus.
In front of this situation she benefited from an opinion in neurology with decision of the neurologists to monitor the patient.
The evolution was marked by the installation of hemodynamic instability at 72 hours of his hospitalization, hence the decision to proceed to a caesarean section for maternal rescue.
The post-diaper period was marked by hospitalization in a neurology environment where she was monitored until stabilization and complete improvement.
Discussion
Stroke is a neurological emergency with very high morbidity and mortality, recent studies have shown that the incidence of stroke, although rare, is increasing in pregnant women. In published research [5-7]. That analysed data from a national hospitalization registry, between 1994 - 1995 and 2006 - 2007, hospitalization rates for stroke increased by 47% and 83% respectively. Summarizing several other studies [8,9], the stroke rate is estimated at 25 - 34 case per 100,000 deliveries, while the incidence of stroke in non-pregnant women 15 - 44 years is 11 per 100,000 women. The study by Kuklina et al [9] also reports that hypertensive disorders have been directly implicated in strokes during pregnancy. Other studies have shown similar results [10,11]. Hypertension is recognized as the number one risk factor for stroke, and it is not an exception in pregnant women. Hypertension during pregnancy may be pre-existing, gestational or secondary to pre-eclampsia or eclampsia, compared to women without hypertension, women with hypertension during pregnancy are six to nine times more likely to have a stroke [11]. The initial evaluation includes a brain scan without injection of contrast medium, it is the radiological examination of choice to highlight intracerebral hemorrhage in the form of diffuse petechiae in the cortex, small subcortical hemorrhagic areas or hematoma. In our patient, the CT scan was performed as a first-line test. This allowed us to highlight the presence of hypodense corticosteroid range under – cortical mainly subcortical bilateral asymmetrical at the level occipito parietal left and parietal right not systematized associated with a left cerebellar intraparenchymal hemorrhage with triventricular hydrocephalus. This imaging was supplemented by a brain MRI whose description was in favor of a PRES complicated syndrome of cerebellar hemorrhagic rearrangements and active triventricular hydrocephalus. The description of lesions made on MRI generally reveals on the FLAIR-weighted sequences confluent areas of posterior hyperintensities that can affect the cerebral cortex (occipital, parietal), adjacent white matter, basal ganglia (thalamus), brainstem and cerebellum. These hyperintense lesions in diffusion (DWI sequences, b1000) have an increased water diffusion coefficient, testifying to a vasogenic edema corresponding to a picture of reversible cerebral encephalopathy (PRES or Posterior Reversible Encephalopathy Syndrome), which can itself be complicated by a Reversible Cerebral Vasoconstriction Syndrome (SVCR) [12,13]. As in our specific case. Intracranial hypertension in eclampsia should be closely managed by antihypertensives and anticonvulsants, including magnesium sulfate [12,13]. Hemorrhagic lesions have a particularly poor prognosis [14]. They are responsible for 40 to 60% of eclamptic deaths. Out of a series of 18 STAUDER patients, two patients with hemorrhagic syndrome progressed favorably and one patient had visual sequelae at a distance from the eclamptic episode [14]. Diffuse cerebral edema also seems to be a factor in poor prognosis. Some authors have found the presence of cerebral edema in 20% of women who died of eclampsia [15,16]. Eclamptic crisis is most often a complication of poorly monitored pregnancies. The most effective strategy for detecting pre-eclampsia is to monitor blood pressure counts during the second and third trimester of pregnancy. Several therapeutic agents are used as preventive measures for eclampsia. Currently, aspirin treatment has shown its effectiveness in terms of prevention. Indeed, a prospective randomized study had shown a significant decrease in the rate of preeclampsia in the group of women with a history of major obstetrics treated with 150 mg/d aspirin and 300 mg/day. In practice, doses of 50 to 100 mg/day are used at the 14th week if there is a pathological history or at the 22nd week if the Doppler is pathological [17,18].
Conclusion
Preeclampsia is still common in developing countries including ours. It is a disease that can lead to eclampsia, responsible for high maternal and infant mortality. The pathophysiology of intracranial lesions is complex associating hypertensive encephalopathy and ischemia secondary to endothelial vascular involvement and cerebral vasospasm. The systematic performance of MRI with diffusion sequences in eclamptics with neurological disorders allows a better diagnostic and prognostic approach of these patients. Intracerebral hemorrhage is a rare but serious complication in pregnant women, several studies are underway to fill knowledge gaps that may be involved in the care of preeclamptic patients with neurological complications. Rapid therapeutic management is necessary in order to control these different processes, avoid their aggravation and obtain a better prognosis.
Declarations
Conflicts of interest: Authors do not declare any conflict of interest.
Authors’ contributions: All authors contributed to the conduct of this work. All authors also declare that they have read and approved the final version of the manuscript.
References
- Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. The Lancet. 2010; 376: 631-644.
- Les morts maternelles en France: Mieux comprendre pour mieux prévenir. 5e rapport de l’Enquête Nationale Confidentielle sur les Morts Maternelles (ENCMM), 2010-2012. Saint-Maurice: Santé publique France. 2017; Disponible à partir de l’URL: www.santepubliquefrance.fr . 4
- PY Ancel, F Goffinet. EPIPAGE 2 Writing Group. Survival and morbidity of preterm children born at 22 trough 34 weeks’ gestation in France in 2011: Results of the EPIPAGE 2 cohort study. JAMA Pediatr. 2015; 169: 230-238.
- Prise en charge multidisciplinaire des formes graves de prééclampsie. Recommandations formaliséesd’experts communes SFAR/CNGOF/SFMP/SFNN. 2009.
- Geographic variation in the incidence of hypertension in pregnancy. World Health Organization International Collaborative Study of Hypertensive Disorders of Pregnancy. Am J Obstet Gynecol. 1988; 158: 80- 83.
- Roberts JM, Pearson G, Cutler J, Lindheimer M. NHLBI Working Group on Research on Hypertension during pregnancy. Summary of the NHLBI Working Group on research on hypertension during pregnancy. Hypertens Dallas Tex. 2003; 41: 437-445.
- Dieckmann WJ. The toxemias of pregnancy, 2nd Edition. St Louis, MO: CV Mosby Co. Israel Journal of Medical Sciences. 1970; 6: 253-266.
- Moodley J. Maternal deaths associated with hypertensive disorders of pregnancy: A population-based study. Hypertens Pregnancy. 2004; 23: 247-256.
- Kuklina EV, Tong X, Bansil P, George MG, Callaghan WM, et al. Trends in pregnancy hospitalizations that included a stroke in the United States from 1994 to 2007: Reasons for concern? Stroke. 2011; 42: 2564-2570.
- James AH, Bushnell CD, Jamison MG, Myers ER. Incidence and risk factors for stroke in pregnancy and the puerperium. Obstet Gynecol. 2005; 106: 509-516.
- Kittner SJ, Stern BJ, Feeser BR, Hebel R, Nagey DA, Buchholz DW, et al. Pregnancy and the risk of stroke. N Engl J Med. 1996; 335: 768-774.
- Lanska DJ, Kryscio RJ. Risk factors for peripartum and postpartum stroke and intracranial venous thrombosis. Stroke. 2000; 31: 1274-1282.
- Duley L, Henderson-Smart DJ, Chou D. Magnesium sulphate versus phenytoin for eclampsia. Cochrane Database Syst Rev. 2010; 10: CD000128.
- Deshaies EM, Boulos AS, Drazin D, Popp AJ. Evidence-based pharmacotherapy for cerebral vasospasm. Neurol Res. 2009; 31: 615-620.
- Thomas SV. Neurological aspects of eclampsia. J Neurol Sci. 1998; 155: 37-43.
- Pourrat O. Pre-éclampsie et éclampsie: Progrès thérapeutiques. Flammarion médecine -sciences - actualités néphrologiques. 2004; 177-189.
- Boufettal H, Moussaïd I, Noun M, Hermas S, Salmi S, Miguil M, et al. Gestational recurrent of ischemic stroke event. Ann Fr Anesth Reanim. 2012; 31: 977-978.
- McDermott M, Miller EC, Rundek T, Hurn PD, Bushnell CD: Preeclampsia: Association with posterior reversible encephalopathy syndrome and stroke. 2018; 4: 524-530.