Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clincal Image - Open Access, Volume 4
From thoracic mass to the diagnosis of esophageal neoplasm:
A case of bizarre metastasis in the chest wall
Sara Costa-Martins*; Sofia Lopes; Inês Vicente; Salete Valente
Centro Hospitalar Universitário Cova da Beira, Alameda Pêro da Covilhã, 6200-251 Covilhã, Castelo Branco, Portugal.
*Corresponding Author : Sara Costa-Martins
Centro Hospitalar Universitário Cova da Beira, Alameda Pêro da Covilhã, 6200-251 Covilhã, Castelo Branco, Portugal.
Ph: +351 915 513 367;
Email: sara.m.costamartins@gmail.com
Received : Jan 28, 2023
Accepted : Feb 15, 2023
Published : Feb 22, 2023
Archived : www.jcimcr.org
Copyright : © Martins SC (2023).
Citation: Martins SC, Lopes S, Vicente I, Valente S. From thoracic mass to the diagnosis of esophageal neoplasm: A case of bizarre metastasis in the chest wall. J Clin Images Med Case Rep. 2023; 4(2): 2297.
Clincal image description
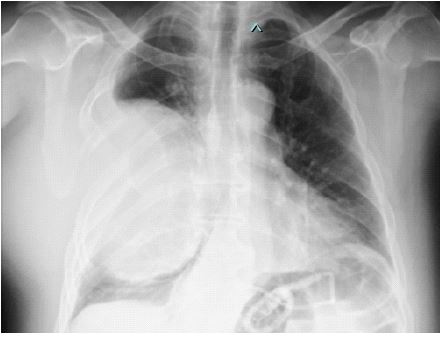
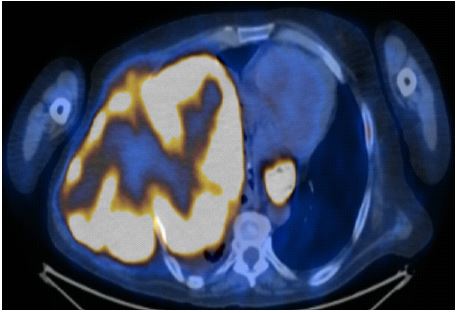
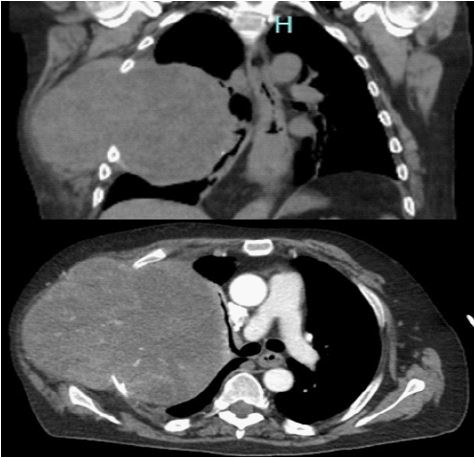
Non-smoker 57-years-old male, with a history of bariatric surgery (gastric banding), was observed due to a right infraaxillary tumefaction, with progressive dimensional increase, anorexia, asthenia, and unquantified weight loss over the past 2 months. He also referred dyspnoea for small efforts and chest pain in orthostatism. No complaints of dysphagia or other gastrointestinal symptoms. On physical examination, he presented a voluminous mass on the right chest wall, stony, adherent to the deep planes and painless on palpation. Analytically with normochromic normocytic anaemia, increase in lactic dehydrogenase 765 U/L, C-reactive protein 18.5 ng/mL and type 1 respiratory failure. Thoracoabdominal Computed Tomography (CT) showed a large soft tissue mass, 22 x 18 x 16 cm, heterogeneous, with an intra and extra-thoracic component, conditioning costal arch destruction and ipsilateral lung collapse, as well as parietal thickening of the distal portion of the oesophagus and esophagogastric junction. An ulcerated invasive neoplasm occupying >75% of that lumen (Siewert type I) was observed by upper digestive endoscopy. F-Fluorodeoxyglucose (FDG) positron emission tomography-CT showed intensely hypermetabolic thickening of the lower third of the esophagus (qSUVmax: 17.0), at the level of the large mass (qSUVmax: 17.0), as well as in isolated lesions (right lower paraesophageal adenopathy (qSUVmax: 5.9) and osteolytic lesion in the 5th left rib (qSUVmax: 13.7)). A percutaneous thoracic biopsy was performed, whose histology was compatible with adenocarcinoma (TTF1, CK7, CK20, CD56, CD99, all negative), sharing the histological and immunohistochemical results of esophageal biopsies. In a multidisciplinary meeting of digestive tumors, the diagnosis of stage IV adenocarcinoma of the distal esophagus was concluded, and the patient was proposed for palliative chemotherapy.
We share this case due to the atypical presentation of an esophageal neoplasia, with a massive metastasis of the chest wall that prompted the start of the diagnostic process, in a patient without gastrointetsinal symptoms.