
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Dr Jekyll and Mr Hyde’ of exocrine gland carcinomas: Breast
adenoid cystic carcinoma - A rare entity
Asmita Suri; Nikhil Talwar*; Moeen; Arvind Ahuja
Department of Surgery, Lady Hardinge Medical College, New Delhi, India.
Department of Pathology*, Atal Bihari Vajpayee Institute of Medical Sciences & Dr RML Hospital, New Delhi, India.
*Corresponding Author : Nikhil Talwar
Department of Surgery Lady Hardinge Medical College, New Delhi – 110001, India.
Ph: 9868392727;
Email: nikhiltalwar@outlook.com
Received : Jan 28, 2023
Accepted : Feb 16, 2023
Published : Feb 23, 2023
Archived : www.jcimcr.org
Copyright : © Talwar N (2023).
Abstract
Primary Adenoid Cystic Carcinoma of Breast (bACC) is an extremely rare salivary gland-like tumor accounting for less than 0.1% of all breast tumors with excellent prognosis. These tumors are generally triple-negative. There is limited data on optimal treatment and management. We herein report a patient who underwent a Modified Radical Mastectomy for carcinoma of the left breast, and the post-operative histopathology revealed bACC.
Citation: Suri A, Talwar N, Moeen, Ahuja A. Dr Jekyll and Mr Hyde’ of exocrine gland carcinomas: Breast adenoid cystic carcinoma - A rare entity. J Clin Images Med Case Rep. 2023; 4(2): 2298.
Introduction
Primary Adenoid Cystic Carcinoma Of Breast (bACC) is an extremely rare salivary gland-like tumor, accounting for less than 0.1% of all breast tumors [1-3]. There is female preponderance with a median age of onset between 50 to 60 years [4]. On histomorphology, it is characterised by a biphasic pattern and consists of a cystic/adenoid part with proliferating glands along with a basaloid myoepithelial portion [5,6]. bACC is generally triple-negative i.e. ER, PR and her 2/neu negative [7,8]. However, unlike the very aggressive typical triple-negative breast tumors, bACC has a favourable prognosis with an excellent 10-year survival rate which ranges from 85 to 100% [9]. We here in report a patient who underwent a Modified Radical Mastectomy for carcinoma of the left breast, and the post-operative histopathology revealed bACC.
Case description/presentation
A 35-year-old female presented with an eighteen-month history of a palpable mass on left breast associated with occasional pain. She underwent a lumpectomy at a private hospital. Histopathological examination was suggestive of IDC. She reported to our Out-Patient Department one month after surgery. Examination revealed a healthy scar of 4 cm in the upper-outer quadrant. No underlying lump was palpable. Opposite breast did not have any lump and there was no axillary metastasis. Her past medical history was unremarkable, and she also denied any family history of breast or ovarian cancer.
The hematological profile and biochemical parameters were within normal limits. Ultrasound revealed a hypoechoic solid, heterogeneous mass. CT scan was suggestive of ill-defined enhancing soft tissue lesion in left breast reaching upto the chest wall. A ground glass nodule of 3.5 mm was noted in the lump. The mammogram was graded BIRADS 6 for suspicious findings of multiple ill-defined is to hyper-dense masses. ECG, ultrasound of the abdomen and chest X-Ray detected no serious abnormality and there was no evidence of distant metastases. Histopathological review of the slides brought by the patient revealed a tumor with features suggestive of IDC. However, a panel Immunohistochemistry stains performed was non-contributory owing to poor tissue fixation. Tru-cut biopsy was done twice from the lump but did not yield a conclusive result. Based on above findings, a diagnosis of carcinoma breast TxNoMx was made. Patient was given 4 cycles of Non-Adjuvant Chemotherapy and then underwent a Modified Radical Mastectomy. On gross inspection, the left mastectomy specimen measured 10 x 10 x 2 cm. On serial slicing, a grey-white mass was identified in the central quadrant measuring 1 x 1 cm, which was 1.5 to 7 cm away from the surrounding margins and overlying skin. The tissue was processed for obtaining paraffin embedded blocks. The histopathological examination revealed epithelial and basaloid myoepithelial cells organised in varying combinations of cribriform, tubular and solid patterns. The cribriform pattern showed was dominant, variably-sized islands of neoplastic cells forming true glandular spaces and pseudo lumens in which basophilic mucoid material was filled. Focal solid areas, with sheets of basaloid cells lacking tubular or microcytic formation were observed. Mitotic count was low (3-4/10 hpf). There were no lymphovascular emboli. All the resected margins and the 10 lymph nodes obtained on serial slicing were free of tumor. On immunohistochemistry, the tumor cells showed variable positivity for CK7, CD117, EMA and p63. The tumor cells were immune-negative for ER, PR and Her 2 neu. Ki-67 labeling index was 3-4 %. After the operation, the patient’s treatment was continued with adjuvant chemotherapy and hormonal therapy.
Discussion
Adenoid Cystic Carcinoma (ACC) was first termed “cylindroma” by Billroth in 1856 due to its characteristic histologic appearance [6]. It is a unique pathological breast entity characterized by a heterogeneous histological appearance that usually occurs in the salivary glands, but is also seen and in other anatomical sites, including the digestive tract, external auditory canal, skin, uterus, lungs, prostate and breast [11]. A previous study using SEER data (1977-2006) showed that the Age-Adjusted Incidence Ratio (AAIR) of bACC is approximately 0.92 per 1 million person-years [9].
In view of it’s rarity, there is a lack of understanding of the occurrence and development of the disease. Diagnosis and treatment modalities for bACC are controversial, but over the years several surgical management options have been considered. Lumpectomy, wide local excision with or without radical radiation, or modified radical mastectomy are performed [12,13]. Unlike most other breast cancers, bACC with it’s low expression of Ki-67, indolent clinical course and low malignant potential, rarely metastasizes to the axillary lymph nodes. Routine axillary dissection is hence not recommended in the management of this disease [12,14]. The term “Dr Jekyll and Mr Hyde of exocrine gland carcinomas” has been used for these tumors as they have an aggressive course when located in the salivary gland with a predilection for metastases while the behave indolently in the breast.
Some studies show an unfavorable increased risk for local recurrence varying from 6% to 37% when treated with local excision or lumpectomy [8]. Adjuvant radiotherapy after the surgical procedure decreases the local recurrence rates [14,12]. Modified radical mastectomy is the most reported surgical procedure for bACC, simply because it used to be the standard treatment for common breast cancers [12]. In the present case, Ki-67 expression was low and the patient’s receptor status was triple negative: (ER, PR and HER-2/neu negative). Modified radical mastectomy was performed which showed no axillary node involvement, thereby suggesting that axillary surgery may be excessive to some extent and could be omitted in patients in the future.
A majority of these cancers cannot be accurately identified based solely on the intraoperative frozen section or routine histopathological evaluation [10]. Other close differentials include Collagen corpuscle disease, Invasive cribriform carcinoma, Cribri form ductal carcinoma in situ, Adenoid invasive ductal carcinoma and Collagenous spherulosis [9]. A panel of immunohistochemicalstains or ultrastructural examination is recommended for proper evaluation.
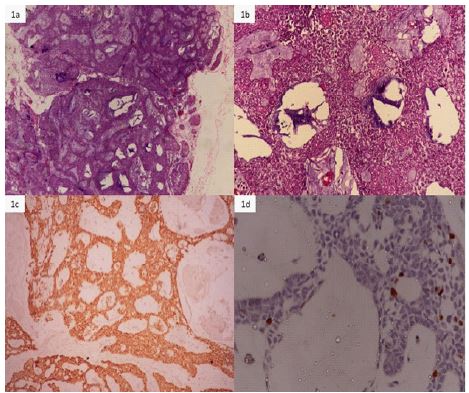
(b) High power showing predominantly monomorphic epithelial cells lining the cystic spaces (H&E, x200).
(c) CK7 IHC showing diffuse membranous positivity X200.
(d) Ki-67 IHC with low LI X 200.
Conclusion
To conclude, bACC is a rare subgroup of low-grade tumors with an indolent clinical behavior that also displays a triple-negative, basal-like phenotype. There is limited data on optimal treatment and management. Owing to both prognostic and predictive implications, large-scale studies with regular review and long-term follow-up arewarranted for development of optimal strategy for personalized therapies. An awareness about this entity is crucial to avoid misdiagnosis and improper treatment.
References
- Glazebrook KN, Reynolds C, Smith RL, Gimenez EI, Boughey JC, et al. Adenoidcystic carcinoma of the breast. AJR Am J Roentgenol. 2010; 194: 1391–1396.
- Miyai K, Schwartz MR, Divatia MK, Anton RC, Park YW, et al. Adenoid cystic carcinoma of breast: Recent advances. World J Clin cases. 2014; 2: 732–741.
- Treitl D, Radkani P, Rizer M, El Hussein S, Paramo JC, et al. Adenoid cystic carcinoma of the breast, 20 years of experience in a single center with review of literature. Breast Cancer. 2018; 25: 28–33.
- Welsh JL, Keeney MG, Hoskin TL, Glazebrook KN, Boughey JC, Shah SS, et al. Is axillary surgery beneficial for patients with adenoid cystic carcinoma of the breast? J Surg Oncol. 2017; 116: 690–695.
- Millar BA, Kerba M, Youngson B, Lockwood GA, Liu FF, et al. The potential role of breast conservation surgery and adjuvant breast radiation for adenoid cystic carcinoma of the breast. Breast Cancer Res Treat. 2004; 87: 225-232.
- Canyilmaz E, Uslu GH, Memış Y, Bahat Z, Yildiz K, et al. Adenoid cystic carsinoma of the breast: A case report and literature review. Oncol Lett. 2014; 7: 1599-1601.
- Marchio C, Weigelt B, Reis-Filho JS. Adenoid cystic carcinomas of the breast and salivary glands (or ‘The strange case of Dr Jekyll and Mr Hyde’ of exocrine gland carcinomas). J Clin Pathol. 2010; 63: 220–228.
- Kim M, Lee D-W, Im J, Suh KJ, Keam B, et al. Adenoid cystic carcinoma of the breast: A case series of six patients and literature review. Cancer Res Treat. 2014; 46: 93–97.
- Ghabach B, Anderson WF, Curtis RE, Huycke MM, Lavigne JA, et al. Adenoid cystic carcinoma of the breast in the United States (1977 to 2006): A population-based cohort study. Breast Cancer Res. 2010; 12: R54.
- Cong Y, Qiao G, Zou H, Lin J, Wang X, et al. Invasive cribriform carcinoma of the breast: A report of nine cases and a review of the literature. Oncol Lett. 2015; 9: 1753–1758.
- Dillon PM, Chakraborty S, Moskaluk CA, Joshi PJ, Thomas CY, et al. Adenoid cystic carcinoma: A review of recent advances, molecular targets, and clinical trials. Head Neck. 2016; 38: 620–627.
- Boujelbene N, Khabir A, Boujelbene N, Jeanneret Sozzi W, Mirimanoff RO, et al. Clinical review - breast adenoid cystic carcinoma. Breast. 2012; 21: 124-127.
- Khanfir K, Kallel A, Villette S, Belkac.mi Y, Vautravers C, et al. Management of adenoid cystic carcinoma of the breast: A Rare Cancer Network study. Int J Radiat Oncol Biol Phys. 2012; 82: 2118-2124.
- Arpino G, Clark GM, Mohsin S, Bardou VJ, Elledge RM, et al. Adenoid cystic carcinoma of the breast. Moleculer markers, treatment, and clinical outcome. Cancer. 2002; 94: 2119-2127.s