
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Varicella zoster virus cerebral vasculopathy without rash accompanied by mucous and bloody diarrhea successfully treated with intravenous acyclovir: A case report
Aleksandar J Ristic 1,3*; Olivera Tamas1, 3; Marija Kovacevic3; Boro Perovic1,2; Maja Stanojevic3; Nikola Vojvodić1,3; Dragoslav Sokić1,3
1Neurology Clinic, University Clinical Center of Serbia, Belgrade, Serbia.
2General Hospital Nikšić, Nikšić, Montengro, Serbia.
3Faculty of Medicine, University of Belgrade, Serbia.
*Corresponding Author : Aleksandar J Ristic
Neurology Clinic, Clinical Center of Serbia Dr Subotićastarijeg 611000 Belgrade, Serbia.
Ph: +381-11-2685-596; Fax: +381-11-2684-577;
Email: aristic@eunet.rs
Received : Feb 02, 2023
Accepted : Feb 23, 2023
Published : Mar 02, 2023
Archived : www.jcimcr.org
Copyright : © Ristić AJ (2023).
Abstract
Introduction: In recent years it has become evident that Varicella Zoster Virus (VZV) reactivation can present as ischemic and hemorrhagic stroke or Gastrointestinal (GI) symptoms in immunocompetent and immunocompromised patients. Both VZV cerebrovascular and visceral manifestations may appear in the absence of a cutaneous rash.
Case report: We present a 49-year-old male patient who presented with recurrent hemorrhagic strokes accompanied by abdominal pain and bloody and mucous in diarrhea without skin lesions following prolonged immunomodulatory therapy (methylprednisolone, azathioprine) due to a decline in platelets in the setting of idiopathicthrombocytopenic purpura. VZV infection was confirmed by virus DNA presence in the cerebrospinal fluid. Both GI and neurological symptoms subsided after a high dose intravenous acyclovir.
Conclusion: Associated neurological and GI symptoms may both be a consequence of VZV reactivation. Knowledge and recognition of divergent and insidious symptoms and sufficienthigh-dose antiviral treatment are crucial in the late VZV disease management.
Keywords: Varicella zoster virus; Recurrent hemorrhagic stroke; Visceral herpes zoster; Bloody and mucous diarrhea.
Abbreviations: VZV: Varicella Zoster Virus; GI: Gastrointestinal; ITP: Idiopathic Thrombocytopenic Purpura; MRI: Magnetic Resonance Imaging; CSF: Cerebrospinal Fluid; CT: Computerized Tomography; Igg: Immunoglobulin G; PCR: Polymerase Chain Reaction; CBC: Complete Blood Count; CNS: Central Nervous System.
Citation: Ristić AJ, Tamaš O, Kovačević M, Perović B, Stanojević M, et al. Varicella zoster virus cerebral vasculopathy without rash accompanied by mucous and bloody diarrhea successfully treated with intravenous acyclovir: A case report. J Clin Images Med Case Rep. 2023; 4(3): 2307.
Introduction
After primary infection (clinically manifested as chickenpox) Varicella Zoster Virus (VZV) establishes persistent infection by becoming latent in human sensory ganglia along the entire neuroaxis [1,2]. Years later VZV can reactivate to cause localized skin lesions – herpes zoster (shingles). However, over the past decades it has become evident that VZV reactivation can also present as ischemic and hemorrhagic stroke produced by VZV vasculopathy in immunocompetent and immunocompromised patients [3-5]. Similarly, VZV reactivation can occur along the Gastrointestinal (GI) tract resulting in epigastric and abdominal pain, bloody stools, and vesiculopapular lesions in the esophagus, intestines or colon [6-8]. Both VZV cerebrovascular and visceral manifestations may appear in the absence of cutaneous rash [9,10].
We report a case of recurrent VZV vasculopathy accompanied by abdominal pain, diarrhea, mucus and blood in stool successfully treated with a high dose intravenous acyclovir.
Case report
A 49-year old male patient, previously diagnosed with Idiopathic Thrombocytopenic Purpura (ITP) and arterial hypertension, started experiencing exacerbations of neurological symptoms one year prior to admission to our inpatient hospital. The first manifestation of the neurological disease was acute headache associated with speech disturbances. Brain Magnetic Resonance Imaging (MRI) showed hemorrhagic infarction in the left parietotemporal region, initially thought to be a possible glial tumor (Figure 1a,1b). The patient was operated on, but histopathology results showed hemorrhage and no signs of tumor. This was followed by transient, predominantly sensory dysphasia, lasting two months. The next exacerbation took place six months after the initial one with epileptic seizures (clonic seizures involving the right half of the face and hand), in the setting of a fever with laboratory values suggesting inflammation, acute speech difficulties, right-sidedweakness and moderate to severe pain in the right upper quadrant. Several weeks later, the patient experienced the presence of mucous and bloody diarrhea. Both neurological exacerbations occurredfollowing prolonged immunomodulatory therapy (methylprednisolone, azathioprine) due to the decline in platelets in the setting of ITP.
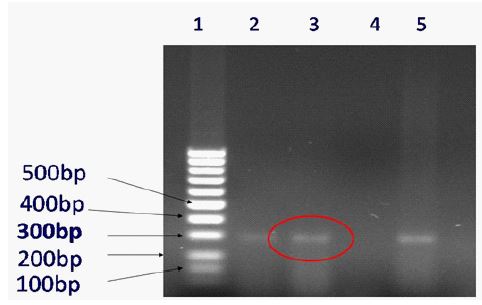
The patient was referred to our hospital and global, predominantly motor aphasia with right-sided hemiparesis was demonstrated. Repeated Cerebrospinal Fluid (CSF) examination showed pleocytosis, (5 cells), hyperproteinorrachia (0.65 g/l), and hypoglycorrhachia (3.2 mmol/l). Brain MRI revealeda new area ofinfarction in the left frontal operculum that underwent hemorrhagic transformation (Figure 1c,1d). Significant vascular abnormalitieswere not identified by CT brain angiography. Viral etiology of the disease was verified by the detection of anti-VZV antibody in CSF, with a significant CSF/serum index for anti-VZV IgG antibodies of 9.3, and bythe detection of VZV DNA in CSF by Polymerase Chain Reaction (PCR) (Figure 2). Zoster lesions were not observed and there was no history of zoster obtained.
DNA was extracted from the cerebrospinal fluid of an immunocompromised patient with small and large vessel vasculopathy due the varicella zoster virus.
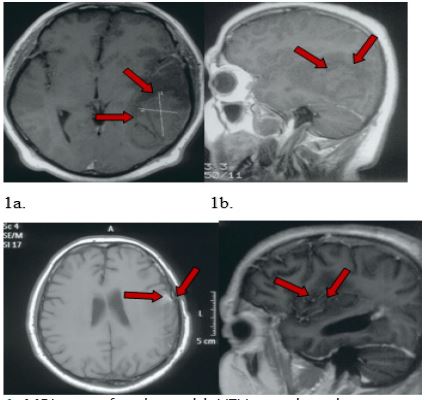
1a. axial, and 1b. sagittal T1W hemorrhagic infarction in the left parietotemporal region, initially thought to be a possible glial tumor.
1c. axial and 1d. sagittal T1W infarction in the left frontal operculum with focal cortical T1 Whyperintensity (hemorrhagic transformation).
The patient received causal treatment with high daily doses of intravenous acyclovir (750 mg tid) for three weeks. This resulted in the significant improvement of his subjective symptoms of abdominal pain and fatigue, full cessation of bloody and mucous diarrhea, and normalization of anemia, hypokalemia, and hypocalcemia (observed through the regular monitoring of laboratory parameters during the time of his hospital stay). The end of the treatment also coincided with the moderate improvement of his neurological status – residual, dominantly motor dysphasia in addition to signs of mild right-sided hemiparesis. At one point, proteinuria/hematuria without changes in the nitrogen balance of bloodwas found. This stopped after the discontinuation of gentamicin initially given to the patient as part of the treatment. Gastroduodenoscopy and colonoscopy were performed after the subsidence of GI problems and did not show any significant lesions in the explored portion. In addition to acyclovir, the patient was also given antihypertensive, gastroprotective, antibiotic, antiepileptic, and antidepressant treatment during the inpatient hospital stay. Throughout the whole period the patient’s level of platelets was within the normal limits. VZV DNA in serumwas negative at discharge.
Discussion
To the best of our knowledge, VZV cerebral vasculopathy accompanied by mucous and bloody diarrhea representing a possible VZV infection of the colon in the absence of the cutaneous rashhas not been reported. Direct evidence of VZV presence in the GI system of our patient is missing. It is important to note that GI diagnostic procedures were performed after the end of causative treatment and following significant clinical improvement. Nevertheless, full cessation of bloody stools, and improvement of blood potassium, calcium and CBC values following high doses of intravenous acyclovir, in the absence of other known causes of colitis, makes the diagnosis of VZV colitis likely. Previous reports of zoster associated with colitis described broad skin lesions in the patient’s left buttock and explained visceral involvement as a consequence of an infected S2 dermatome [8]. However, visceral symptoms in our case could be due to colon infection at any location, not related to brain lesions.
VZV reactivation with subsequent transaxonal spread to cranial blood vessels and transmural spread with pathological wall remodeling is the most probable mechanism in vascular involvement [11]. VZV vasculopathy in the CNS affects large and small cerebral vessels in immunocompetent or immunocompromised patients respectively [12,13]. In some patients, both large and small vessels are involved. A chronic course, and protean neurologic features, without recent history of zoster, as was the casewith our patient, makes the diagnosis challenging [10].
Long-term prednisone and cyclophosphamide treatment of thrombocytopenia preceded both neurological exacerbations in our case. An instructive case illustrated an immunocompromised patient demonstrating many clinical, imaging and CSF features seen in VZV vasculopathy, who was hospitalized for months, treated with steroids and cyclophosphamide and who in the end deteriorated and passed [14,15]. Thus, immunomodulatory treatment of our patient significantly contributed to the worsening of symptoms and heterogeneity of clinical features. However, the role of thrombocytopenia in our case is not clear.
Finally, as in previous reports [9,16], we observed a dramatic improvement of clinical features three weeks after the acyclovir treatment in addition to negative serological results at the time of discharge. We initiated antiviral agents late in the course of VZV vasculopathy associated with visceral varicella zoster disease. Although early treatment of acyclovir is advocated as effective [9], we report a favorable treatment response almost a year after initial neurological presentation.
Conclusion
Combined neurological and gastrointestinal symptoms may be due to VZV reactivation. The detection of anti VZV IgG antibodies and VZV DNA can support that diagnosis even in a patient without skin changes. Establishing the diagnosis quickly and precisely aids inthe effective treatment of VZV vasculopathy.
Declarations
Authors have no conflicts of interest to disclose.
Acknowledgment: This work was partly supportedby the Republic of Serbia, Ministry of Education and Science, project No. 175024.
References
- Gilden DH, VafaiA, Shtram Y, Becker Y, Devlin M, Wellish M, et al. Varicella-zoster virus DNA in human sensory ganglia. Nature. 1983; 306: 478-480.
- Hyman RW, Ecker JR and Tenser RB. Varicella-zoster virus RNA in human trigeminal ganglia. Lancet. 1983; 2: 814-816.
- Cravioto H and Feigin I. Noninfectious granulomatous angiitis with a predilection for the nervous system. Neurology. 1959; 9: 599-609.
- Nagel MA, Cohrs RJ, Mahalingam R, Wellish MC, Forghani B, et al. The varicella zoster virus vasculopathies: clinical, CSF, imaging, and virologic features. Neurology. 2008; 70: 853-860.
- Galetta KM and Gilden D. Zeroing in on zoster: A tale of many disorders produced by one virus. J Neurol Sci. 2015; 358: 38-45.
- Ryle JA. Visceral herpeszoster. British Medical Journal. 1932; 1: 726.
- de Jong MD, Weel JF, van Oers MH, Boom R, Wertheim-van Dillen PM, et al. Molecular diagnosis of visceral herpes zoster. Lancet. 2001; 357: 2101–2102.
- Okimura H, Muto M, Ichimiya M, Mogami S, Takahata H, Asagami C, et al. A case of herpes zoster associated with colitis. J Dermatol. 1996; 23: 631-634.
- Gilden D, Cohrs RJ, Mahalingam R, Nagel MA. Varicella zoster virus vasculopathies: Diverse clinical manifestations, laboratory features, pathogenesis, and treatment. Lancet Neurol. 2009; 8: 731-740.
- Gilden DH, Dueland AN, Devlin ME, Mahalingam R, Cohrs R, et al. Varicella-zoster virus reactivation without rash. J Infect Dis. 1992; 166: S30-S34.
- Nagel MA and Bubak AN. Varicella Zoster Virus Vasculopathy. J Infect Dis. 2018; 218: S107-S112.
- Kleinschmidt-DeMasters BK, Amlie-Lefond C and Gilden DH. The patterns of varicella zoster virus encephalitis. Hum Pathol. 1996; 27: 927-938.
- Gilden DH, Mahalingam R, Cohrs RJ, Kleinschmidt-DeMasters BK and Forghani B. The protean manifestations of varicella-zoster virus vasculopathy. J Neurovirol. 2002; 8 :75-79.
- Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 5-1995. A 73-year-old man with focal brain lesions and peripheral-nerve disease [published correction appears in N Engl J Med. 1995; 332: 1527. N Engl J Med. 1995; 332: 452-459.
- Gilden DH, Kleinschmidt-De Masters BK, Wellish M, Hedley-Whyte ET, Rentier B, Mahalingam R, et al. Varicella zoster virus, a cause of waxing and waning vasculitis: The New England Journal of Medicine case 5-1995 revisited. Neurology. 1996; 47: 1441-1446.
- Ishizawa J, Fujita H, Iguchi M, Tachibana T, Taguchi J, et al. Quantification of circulating varicella-zoster virus DNA for follow-up in a case of visceral varicella-zoster infection ameliorated with intravenous acyclovir. Int J Hematol. 2007; 85: 242-245.