
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Erdheim-Chester disease with a late onset cardiovascular manifestations: A case report
Bahman Rasuliˡ; Elahe Zaremehrjardi2
1Jame Jam Imaging Center, Tehran University of Medical Sciences, Shahriar, Tehran, Iran.
2Imam Khomeini Hospital, Medical Faculty of Tehran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Rasuli Bahman
Jame Jam Imaging Center, Tehran University of Medical Sciences, Shahriar, Tehran, Iran.
Email: bahman_rasuli@yahoo.com
Received : Feb 13, 2023
Accepted : Mar 01, 2023
Published : Mar 08, 2023
Archived : www.jcimcr.org
Copyright : © Bahman R (2023).
Abstract
Introduction: Erdheim-Chester disease (ECD) is an uncommon non-Langerhans cell histiocytosis. Bilateral symmetric sclerosis of the long bones and probable multiorgan involvement are the main manifestations of this condition. Here, we report a case of ECD showing diffuse thickening of the aorta’s entire wall and pericardial effusion.
Case presentation: We represent the case of a 50-year-old man with a diagnosis of ECD who was admitted because of dyspnea, chest tightness and slight limitation of physical activity with NYHA II which started 4 months ago and has gotten progressively worse. He has been observed by the Hematology team since 2004 with bilateral hydronephrosis, retroperitoneal fibrosis, and bone involvement. Echocardiography revealed pericardial effusion. Computed tomography (CT) revealed pericardial effusion and diffuse thickening of the aorta’s entire wall with a narrowing area in the infra-renal section. Based on patients’ clinical and imaging findings and considering the multisystem manifestations of ECD, cardiovascular system involvement although with a late onset but was the further involvement of the disease.
Conclusion: Cardiovascular representations of ECD are associated with a poor prognosis and more than half of the patients are frequently affected. Aortic infiltration and pericardial effusion are the most common conditions.
Keywords: Erdheim-Chester disease; Pericardial effusion; Aorta wall thickening.
Citation: Bahman R, Elahe Z. Erdheim-Chester disease with a late onset cardiovascular manifestations: A case report. J Clin Images Med Case Rep. 2023; 4(3): 2315.
Introduction
Erdheim-Chester Disease (ECD) is a very rare, non-familial, xanthogranulomatous non-Langerhans cell histiocytosis of an unidentified origin. William Chester and his tutor, Jakob Erdheim (a Viennese pathologist), first depicted this condition in 1930 [1]. However, the precise etiology of ECD has not been documented. ECD is understood to affect multiple organs, with various manifestations of highly variable severity. Most patients with ECD are diagnosed between the ages of 40 and 70 years, with a marginal male predilection [2]. The classic presenting manifestation of ECD is bone pain, followed by bilateral, symmetric metaphyseal, and diaphyseal multifocal sclerosis of the long bones. In addition to the long bones, the central nervous system (CNS), cardiovascular system, lung, pancreas, breast, and testicles can also be involved. Cardiovascular involvement occurs in various ways, with periaortic fibrosis being the most common presentation, with a tomographic finding typically defined as a “coated aorta”, which is asymptomatic in most patients [3]. The presence of cardiovascular system impairment is associated with a worse prognosis and is a major cause of death in this disease [4-6]. Identification of the cardiovascular involvements is of the utmost importance for the adequate management of these patients. Herein, we demonstrate the case of a 50-year-old man with ECD, who presented with dyspnea, chest tightness, and slight limitation of physical activity with NYHA II.
Case report
A 50-year-old male patient, with no prior comorbidities, was observed by the Hematology team with a diagnosis of ECD since 2004 with bilateral hydronephrosis, retroperitoneal fibrosis, and bone involvements. His diagnosis was confirmed through a right femur bone biopsy with CD68+ histiocyte, negative S-100, started treatment with interferon and prednisone. In 2022, he developed dyspnea, chest tightness and a slight limitation of physical activity with NYHA II which started 4 months ago. Besides, he complained of gradually increased bilateral flank and lower limb pains in the recent 6 months which are not completely alleviated by analgesic drugs.
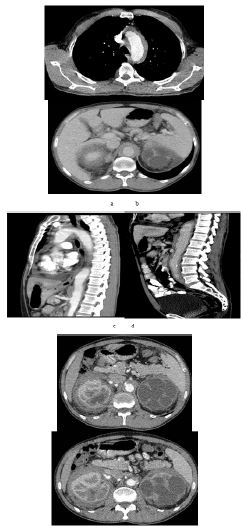
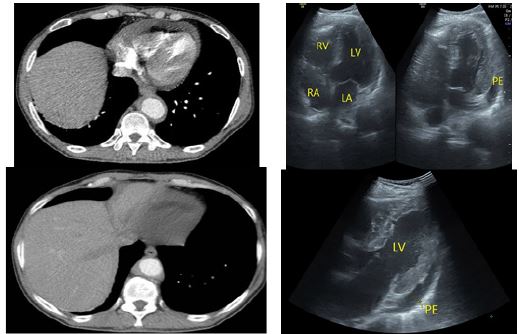
Physical examination and biochemical screening, except for blood pressure 142/94 mmHg, CRP (55 mg/dL), and erythrocyte sedimentation rate (ESR: 40 mm/h), indicated no abnormalities. On the next day, a chest and abdominopelvic Computed Tomography (CT) scan was conducted. It showed hypoattenuating tissues with extensive involvement of the thoracoabdominal aorta and its branches as well as characterized by the narrowing of the aorta in the emergence region of the renal arteries (Figure 1). A Thoracic CT scan and Transthoracic Echocardiography (TTE) also showed a discreet pericardial effusion (Figure 2).
Discussion
ECD is an uncommon, non-inherited, multiorgan non-Langerhans cell histiocytosis, with unrecognized pathogenesis. It is generally diagnosed in middle-aged people, with a marginal male preference. Pathologically, this disease is described by the infiltration of lipid-laden histiocytes, Touton giant cells, and a variable extent of background fibrosis. In the immunohistochemical tissue study, the histiocytes stained positive for CD68, whereas S-100 and CD1 were negative, unlike Langerhans Cell Histiocytosis (LCH). Moreover, it is associated with BRAF V600E mutations [7]. The coexistence of ECD with LCH with double infiltration of various cells has been also documented [8-10].
ECD usually contributes with a range of non-specific manifestations; however, the most common presenting symptom is bone pain, followed by bilateral, symmetric metaphyseal, and diaphyseal sclerosis of the long bones in the majority of patients [11].
Also, more than half of ECD patients have extra skeletal manifestations, such as retroperitoneal fibrosis, orbital infiltration, interstitial lung disease, bilateral adrenal involvement, testicular infiltration, breast, central nervous system, and/or cardiovascular system involvement [12,13].
The prognosis of ECD was reported as poor, with 57% of patients dying after an average follow-up of 32 months [4].
Cardiac involvement is the foremost reason for death in ECD and most of the time, it is asymptomatic. Almost 60% of patients with ECD die because of cardiovascular complications [6,14]. The cardiologist’s knowledge of this disease allows an early diagnosis of these condition.
The most common cardiovascular finding of ECD is seen in the pericardium as pericardial effusion and was reported in 40–45% of patients, like our case. Pericardial effusion can be thoroughly asymptomatic or rarely associated with cardiac tamponade and pericarditis [15,16].
The most characteristic cardiovascular finding of ECD is circumferential infiltration of the aortic wall which can be detectable in a CT scan creating a “coated aorta “appearance and as seen in our case [3,6,17].
Besides, ECD may involve the cardiac myocardium, cardiac valves, coronary arteries, and conduction system [15,18].
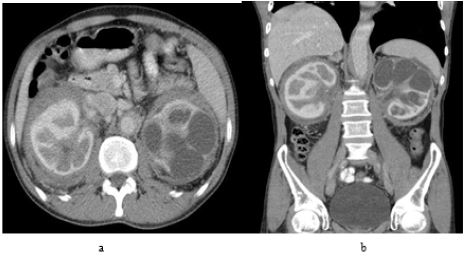

Moreover, an aggressive infiltration of the retroperitoneal structures including the adrenals and kidneys creates a “hairy kidney” appearance (Figure 3). Further radiographic skeletal survey, based on the patient’s irritating bone pain was carried out, which characterized diffuse sclerosis in the long bones of the lower limbs (Figure 4).
ECD with atrial involvement, often as a pseudotumor, affects mostly the atrial posterior wall, often projecting into the atrium. Another observed lesion is the infiltration of the right atrioventricular sulcus, where the tissue usually encircles or infiltrates the right coronary artery [19].
Perivascular infiltration of the thoracoabdominal aorta main branches also appears in the brachiocephalic trunk, left carotid artery, left subclavian artery, coronary arteries, pulmonary trunk, celiac trunk, superior mesenteric artery, and renal arteries [20]. The clinical presentation depends on which artery is involved and its degree of stenosis. Cerebral ischemia may occur due to carotid involvement, and myocardial infarction due to coronary involvement. Renal artery involvement occurs in approximately 20% of cases [5,20] and may result in stenosis of these vessels and renovascular hypertension. Treatment is performed through angioplasty and stenting.
In our case, the recent clinical manifestations were related to the entering of the disease toward the new stage presenting with extensive cardiovascular involvement although late onset in opposition to similar studies and after a long time under observation and conservative treatment and predicting a poor prognosis in the literature [6,14-18].
For this rare and complex disease, clinicians must know the main features of the disease so that they can conduct an early and comprehensive diagnostic investigation.
Conclusion
We report a patient with ECD presenting as pericardial effusion, circumferential infiltration of the aorta and its branches, retroperitoneal fibrosis, and multifocal bone lesions. ECD is an uncommon, non-familial, multisystem, non-Langerhans cell histiocytosis, with various manifestations of highly variable severity. Cardiovascular involvement as an extra skeletal manifestation also occurs and predicts a poor prognosis.
References
- Tran TA, Fabre M, Pariente D, Craiu I, Haroche J, et al. Erdheim-Chester disease in childhood: a challenging diagnosis and treatment. J Pediatr Hematol Oncol. 2009; 31: 782-786.
- Arnaud L, Hervier B, Nelly A, Neel A, Hamidou MA, et al. CNS involvement and treatment with interferon-α are independent prognostic factors in Erdheim-Chester disease: a multicenter survival analysis of 53 patients. Blood. 2011; 117: 2778-2782.
- Roei D, Manevich-Mazor M, Shoenfeld Y. Erdheim-Chester Disease: a comprehensive review of the literature. Orphanet J Rare Dis. 2013; 8: 137.
- Diamond EL, Dagna L, Hyman DM, Cavalli G, Janku F, et al. Consensus guidelines for the diagnosis and clinical management of Erdheim-Chester disease. Blood. 2014; 124: 483-492.
- Haroche J, Amoura Z, Dion E, Wechsler B, Costedoat-Chalumeau N, et al. Cardiovascular involvement, an overlooked feature of Erdheim-Chester disease: report of 6 new cases and a literature review. Medicine (Baltimore). 2004; 83: 371-392.
- Haroche J, Cluzel P, Toledano D, Montalescot G, Touitou D, et al. Images in cardiovascular medicine. Cardiac involvement in Erdheim-Chester disease: magnetic resonance and computed tomographic scan imaging in a monocentric series of 37 patients. Circulation. 2009; 119: e597–598.
- Breuil V, Brocq O, Pellegrino C, Grimaud A, Euller-Ziegler L. Erdheim-Chester disease: typical radiological bone features for a rare xanthogranulomatosis. Ann Rheum Dis. 2002; 61: 199-200.
- Verdalles U, Goicoechea M, Garcia de Vinuesa S, Mosse A, Luno J. Erdheim-Chester disease: a rare cause of renal failure. Nephrol Dial Transplant. 2007; 22: 1776-1777.
- Myra C, Sloper L, Tighe PJ, McIntosh RS, Stevens SE, et al. Treatment of Erdheim-Chester disease with cladribine: a rational approach. Br J Ophthalmol. 2004; 88: 844-847.
- Drier A, Haroche J, Savatovsky J, Godeneche G, Dormont D, et al. Cerebral, facial, and orbital involvement in Erdheim-Chester disease: CT and MR imaging findings. Radiology. 2010; 255: 586-594.
- Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D, Wechsler J, Brun B, et al. Erdheim-Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine (Baltimore). 1996; 75: 157-169.
- Pan A, Doyle T, Schlup M, Lubcke R, Schultz M. Unusual manifestation of Erdheim-Chester disease. BMC Gastroenterol. 2011; 11: 77.
- Rasuli B, Shooshtarizadeh T, Hashemi S. A Case of Erdheim-Chester Disease with Omental Caking Initially Mistaken for a Malignancy. Iran J Radiol. 2022; 19.
- Alharthi MS, Calleja A, Panse P, Appleton C, Jaroszewski DE, et al. Multimodality imaging showing complete cardiovascular involvement by Erdheim-Chester disease. Eur J Echocardiogr 2010; 11: E25.
- Costa I, Abdo A, Bittar C et al. Cardiovascular Manifestations of Erdheim-Chester’s Disease: A Case Series. Arq Bras Cardiol. 2018; 111: 852-855.
- Vaglio A, Corradi D, Maestri R, Callegari S, Buzio C, et al. Pericarditis heralding Erdheim-Chester disease. Circulation. 2008; 118: e511-512.
- Serratrice J, Granel B, De Roux C, Pellissier JF, Swiader L, et al. “Coated aorta”: a new sign of Erdheim-Chester disease. J Rheumatol. 2000; 27: 1550-1553.
- Ghotra AS, Thompson K, Lopez-Mattei J, Bawa D, Hernandez R, et al. Cardiovascular manifestations of Erdheim-Chester disease. Echocardiography. 2019; 36: 229-236.
- Gianfreda D, Palumbo AA, Rossi E, Buttarelli L, Manari G, et al. Cardiac involvement in Erdheim-Chester disease: an MRI study. Blood. 2016; 128: 2468-2471.
- Haroche J, Arnaud L, Amoura Z, Cohen-Aulbart F, Hervier B, et al. Erdheim-Chester Disease. Curr Rheumatol Rep. 2014; 16: 412.