
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Extranodal NK/T-Cell lymphoma with Behcet’s syndrome: A case report
Hongjia Du1; Liang Wang1; Jiarui Hu1*; Jing Zhu1; Juan Liu2; Haiyan Gao3; Jiang Su1*
1Department of Rheumatology and Immunology, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu 610072, China.
2Department of Pathology, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu 610072, China.
3Department of Nuclear Medicine, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, Chengdu 610072, China.
*Corresponding Author : Jiang Su
Department of Rheumatology and Immunology, Sichuan Provincial People’s Hospital, University of Electronic Science and Technology of China, No.32 The First Ring Road West 2, Chengdu 610072, China.
Email: sujiangxy@126.com
Received : Feb 14, 2023
Accepted : Mar 07, 2023
Published : Mar 14, 2023
Archived : www.jcimcr.org
Copyright : © Su J (2023).
Abstract
Extranodal natural killer cell (NK)/T-cell lymphoma (ENKL) is a rare type of non-Hodgkin’s lymphoma, accounting for 5%-10% of total NHL cases. ENKL with Behcet’s Syndrome (BS) is even rarer. This paper reports the diagnosis and treatment of a patient of ENKL with BS.
Keywords: NKT Cell; Lymphoma; Behcet’s syndrome; Nasal obstruction; Fever; Case report.
Citation: Du H, Wang L, Hu J, Zhu J, Su J, et al. Extranodal NK/T-Cell lymphoma with Behcet’s syndrome: A case report. J Clin Images Med Case Rep. 2023; 4(3): 2324.
Introduction
Behcet’s Syndrome (BS), also known as Behcet’s disease, is a systemic immune system disease with vasculitis as its basic pathological manifestation, which can affect joints, blood vessels, heart, nerves, and other systems, mainly manifested as oral and perineal ulcers, erythema nodules of lower limbs, eye iritis, esophageal ulcers, small intestine or colon ulcers, joint swelling and pain, etc. [1]. Extranodal natural killer cell (NK)/T-cell lymphoma (ENKL) is a type of non-Hodgkin’s lymphoma, which originates from NK/T cells and mostly occurs in the nasal cavity, paranasal sinuses, and nasopharynx [2,3]. The nasal cavity is the most common site. ENKL is rare, but ENKL with BS is even rarer, which is easily misdiagnosed clinically. In order to deepen the clinician’s understanding of the disease, reduce misdiagnosis and mistreatment, and miss the best treatment period, here, we present a case of ENKL associated with BS.
Case report
A 39-year-old, Chinese man, presented to our hospital with a complaint of nasal obstruction for 3 mo. Symptoms started 3 mo before presentation with dizziness and recurrent fever (up to 39.80C). He had recurrent multiple arterial occlusions in both lower extremities for 9 years. He had a history of 2 surgeries of lower limb vascular bypass graft due to noticeable swelling and pain in his left lower limb, with skin ulceration and gangrene gradually appearing 3 years ago. Half a month after the operations, the pain in the left lower limb gradually worsened, making walking difficult. The ulcer surface of the left lower limb mainly consisted of the left ankle joint gradually expanding. Therefore, he received autologous hematopoietic stem cell transplantation 2 years ago, but the pain in the left lower limb did not alleviate, and the ulcer surface gradually expanded after discharge. Due to the increase in lower limb ulceration and gangrene, he had a history of upper middle leg amputation of the left lower limb 1 year ago. Subsequently, he was diagnosed as BS due to oral ulcer (more than 3 times a year), nodular erythema, pseudofolliculitis, and arteriovenous thrombosis in both lower extremities. Throughout treatment, the patient was on long-term oral warfarin, aspirin, cilostazol, diclofenac, prednisone acetate and cyclophosphamide (cumulative dose 20 g), and azathioprine. The patient denied any relevant family history.
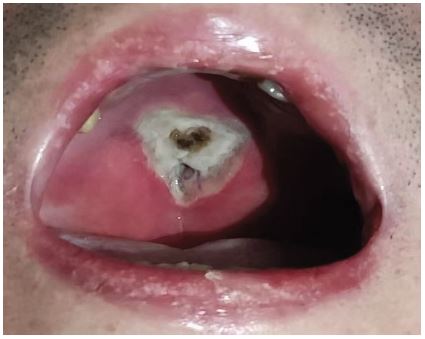
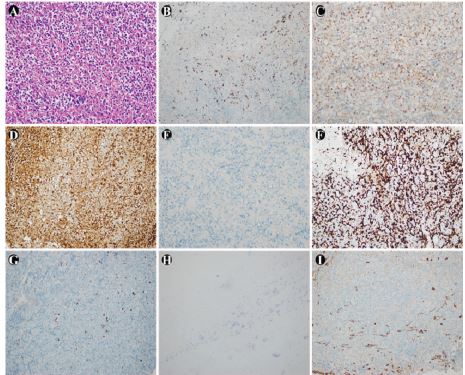
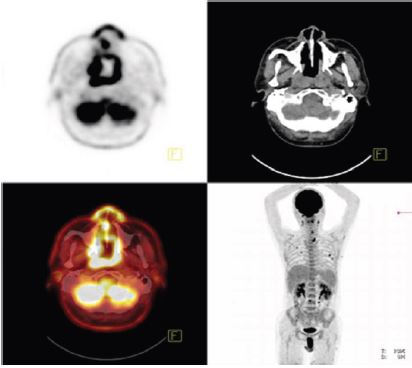
Physical examination revealed a moon face, pharyngeal hyperemia, and a giant invasive palatal ulcer with bone destruction (Figure 1). Pathogenic examination showed that the double bottle blood culture of carbapenemase-resistant Enterobacteriaceae (Klebsiella pneumonia), Candida albicans, and GM were positive. Tumor markers indicated that Neuron-Specific Enolase (NSE) was 34.69 ng/mL (reference, 0-20) and glycogen antigen 125 (CA125) was 39 U/mL (reference, 0-24). Bone marrow cytomorphologic examination revealed that granular erythropoiesis was active, and hemophilia was found. Intranasal soft tissue biopsy showed lymphoid hyperplasia with necrosis and immunohistochemistry revealed CK (-), PAX-5 (-), CD3 (+), TIA-1 (+), GranB (+), CD56 (+), CD8 (a little+), CD21 (-), CD4 (-), Ki-67 (approximately 80%+), EBER (+) (Figure 2), supporting extranodal NK/T-cell lymphoma, nasal type (WHO invasive). 18F-FDG-PET/CT showed thickening of nasopharynx mucosa and significant abnormal activity of FDG metabolism, considering the involvement of lymphoma (Figure 3).
The patient was diagnosed with ENKL, nasal type with BS. After admission, the patient continued treatment with anti-infective drugs, blood transfusion, leukocytosis drugs, and antibiotics and received chemotherapy of gemcitabine combined with oxaliplatin, dexamethasone, and L-asparaginase. Unfortunately, he developed severe agranulocytosis with fever, refractory hypokalemia, and sepsis during chemotherapy, resulting in his death.
Discussion
ENKL, as a rare type of non-Hodgkin’s lymphoma, is the most common type among indigenous people in Asia and Central and South America, accounting for 5%-10% of total NHL cases [4-9]. ENKL mainly occurs in men with a median age of 52 years [5]. Its clinical manifestations are characterized by progressive destruction of the midline of the face, and it can be diagnosed by evaluating biopsy samples from the affected area. Studies have confirmed that the presence of NK/T cell markers and EBV is the key to diagnosis [10].
BS can be combined with other connective tissue diseases. Black and other researchers [11-13] conducted a meta-analysis on the relationship between systemic lupus erythematosus, rheumatoid arthritis, Sjogren’s syndrome, and malignant lymphoma. The results showed that the probability of lymphoma in these three types of patients was higher than that in ordinary healthy people. However, the relationship between BS and lymphoma is still unclear. The majority of lymphoma misdiagnosed as BS in relevant reports is due to the similarity in clinical manifestations (such as oral ulcer, fever, etc.), which makes it challenging to make a precise diagnosis. The types of BS complicated with lymphoma are diverse, and the involved sites are different. The majority of them are non-Hodgkin’s lymphoma. There are only 3 cases of Hodgkin’s lymphoma, which are mixed cell type, tuberous sclerosis type, and nodular lymphocyte type [14-16] Based on the domestic and foreign literature, we reported that ENKL with BS is very rare, and only 5 cases have been reported globally [17-21]. The patient scored 2 points for oral ulcer, 1 point for skin damage, and 1 point for vascular manifestations, totaling 4 points, meeting the 2014 International Criteria for Behcet’s Disease [22]. At the initial stage, the patient suffered from the amputation of the left lower limb due to repeated arterial and venous thrombosis of the lower limb due to a lack of standardized diagnosis and treatment. After treatment with glucocorticoid immunosuppressant, the condition was gradually controlled. During the continuous maintenance treatment, the patient was hospitalized again with nasopharyngeal lesions and fever, which were all unprecedented manifestations. Therefore, it was considered that this disease had nothing to do with BS. Finally, NK/T cell lymphoma was confirmed by tissue biopsy, which was considered as BS complication.
Huang Qin and others [23-29] analyzed the possible mechanism of BS complicated with lymphoma, which may be related to the disorder of immune mechanism, EB virus infection, and the application of immunosuppressants (such as colchicine, cyclophosphamide, and nitrogen mustard phenylbutyrate). While cyclophosphamide is used for BS patients with poor effects of other treatment schemes, long-term use of cyclophosphamide and other alkylating agents may lead to secondary factors of lymphoma, but treatment-related lymphoma in autoimmune diseases has not been confirmed [30]. In our case, BS needed to be better controlled. The patient accumulated 20 g of cyclophosphamide and suffered from lymphoma due to EB virus infection. The use of cyclophosphamide may be involved in the pathogenesis of secondary Extranodal NK/T-cell lymphoma [31-33].
In the course of diagnosis and treatment, the patient has an unexplained ulcer surface, enlarged lymph node, and enlarged parotid gland, accompanied by fever, hormone, and immunosuppressive drugs are ineffective [21], so it is integral to be alert to the possibility of ENKL with BS.
ENKL with BS is rare and is easily misdiagnosed. Clinicians should improve the screening rate of EBV and timely and repeated pathological biopsy for early detection of ENKL complicated with BS, so as to avoid delaying the disease. In addition, long-term use of immunosuppressants is a high-risk group for the occurrence of drug-resistant bacteria. Active screening of colonized bacteria and early rational use of antibiotics to prevent severe infection, and correct evaluation of chemotherapy programs and doses cannot be ignored for the prognosis of patients.
Declarations
Acknowledgements: We would like to thank our patient for participating in this study.
Statement of ethics: Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Ethical review board: The authors declare that they have followed the protocols of their work center on the publication patient data.
Informed consent statement: Informed written consent was obtained from family member of the patient for publication of this report and any accompanying images.
Conflict-of-interest statement: All authors declare that they have no conflict of interest to disclose.
Funding: The authors declare have no commercial or financial relationship with any sponsor, or direct professional relationship with it.
CARE Checklist (2016) statement: All authors have read the CARE Checklist (2016), and this manuscript was prepared and revised according to the CARE Checklist (2016).
References
- Behçet H, Matteson EL. On relapsing, aphthous ulcers of the mouth, eye and genitalia caused by a virus. 1937. Clinical and experimental rheumatology. 2010; 28: S2-5.
- Jaffe ES, Swerdlow S, Campo E, Pileri SA, Wardiman JW. WHO Classification of Tumours of the Haematopoietic and Lymphoid Tissues. Lyon:International Agency for Research on Cancer. 2008; 68-71.
- Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016; 127: 2375-2390.
- Jaffe ES, Chan JK, Su IJ, Frizzera G, Mori S, et al. Report of the Workshop on Nasal and Related Extranodal Angiocentric T/Natural Killer Cell Lymphomas. Definitions, differential diagnosis, and epidemiology. The American journal of surgical pathology. 1996; 20: 103-111.
- Au WY, Weisenburger DD, Intragumtornchai T, Nakamura S, Kim WS, Sng I, et al. Clinical differences between nasal and extranasal natural killer/T-cell lymphoma: a study of 136 cases from the International Peripheral T-Cell Lymphoma Project. Blood. 2009; 113: 3931-3937.
- Au WY, Ma SY, Chim CS, Choy C, Loong F, et al. Clinicopathologic features and treatment outcome of mature T-cell and natural killer-cell lymphomas diagnosed according to the World Health Organization classification scheme: a single center experience of 10 years. Annals of oncology : official journal of the European Society for Medical Oncology. 2005; 16: 206-214.
- Laurini JA, Perry AM, Boilesen E, Diebold J, Maclennan KA, et al. Classification of non-Hodgkin lymphoma in Central and South America: a review of 1028 cases. Blood. 2012; 120: 4795-4801.
- Adams SV, Newcomb PA, Shustov AR. Racial Patterns of Peripheral T-Cell Lymphoma Incidence and Survival in the United States. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2016; 34: 963-971.
- Chim CS, Ma SY, Au WY, Choy C, Lie AK, et al. Primary nasal natural killer cell lymphoma: long-term treatment outcome and relationship with the International Prognostic Index. Blood. 2004; 103: 216-221.
- Kanavaros P, Lescs MC, Brière J, Divine M, Galateau F, Joab I, et al. Nasal T-cell lymphoma: a clinicopathologic entity associated with peculiar phenotype and with Epstein-Barr virus. Blood. 1993; 81: 2688-2695.
- Black KA, Zilko PJ, Dawkins RL, Armstrong BK, Mastaglia GL. Cancer in connective tissue disease. Arthritis and rheumatism. 1982; 25: 1130-1133.
- Canoso JJ, Cohen AS. Malignancy in a series of 70 patients with systemic lupus erythematosus. Arthritis and rheumatism. 1974; 17: 383-390.
- B E B. Dermatomyositis and malignancy. A review of the literature. Annals of internal medicine. 1976; 84: 68-76.
- Kawamoto S, Terada H, Niikura H, Kumasaka T, Saiki S. [Hodgkin’s disease associated with Behçet’s disease]. [Rinsho ketsueki] The Japanese journal of clinical hematology. 1992; 33: 211-215.
- Cengiz M, Altundag MK, Zorlu AF, Güllü IH, Ozyar E, et al. Malignancy in Behçet’s disease: a report of 13 cases and a review of the literature. Clinical rheumatology. 2001; 20: 239-244.
- Meydan AD, Gürsel B, Özbek N, Can B, Kandemir B. Malignant lymphoma associated with Behçet’s disease: A report of 2 cases. Turkish journal of haematology: official journal of Turkish Society of Haematology. 2011; 28: 327-34.
- Ahn JK, Oh JM, Lee J, Koh EM, Cha HS. Behcet’s disease associated with malignancy in Korea: a single center experience. Rheumatology international. 2010; 30: 831-835.
- Lee H, Kim SH, Lee SW, Zheng Z, Bang D, Kim DY. A case of extranodal natural killer/T-cell lymphoma mimicking refractory Behçet’s disease. Acta dermato-venereologica. 2015; 95: 491-492.
- Huang Q, Lai W, Yang M. Behcet’s disease complicated by malignant lymphoma: a case report and literature review. Journal of Southern Medical University. 2013; 33: 934-936.
- Mengjun P, Yufeng Q, Zhenyi Z, Pan Z, Mengyun Z, et al. Behcet’s disease with lymphoma: a case report. Chinese Journal of Rheumatology. 2015; 5: 345-346.
- Pan Z, Jing T, jin W. A case of Behcet’s disease complicated with extranodal NK/T-cell lymphoma. West China Medical Journal. 2014; 29: 1227-1228.
- Kalra S, Silman A, Akman-Demir G, Bohlega S, Borhani-Haghighi A, et al. Diagnosis and management of Neuro-Behçet’s disease: international consensus recommendations. Journal of neurology. 2014; 261: 1662-1676.
- Houman MH, Ben Ghorbel I, B’Chir-Hamzaoui S, Lamloum M, Kchir N, et al. [Intestinal lymphoma associated with Behçet disease]. Annales de medecine interne. 2001; 152: 415-418.
- Zintzaras E, Voulgarelis M, Moutsopoulos HM. The risk of lymphoma development in autoimmune diseases: a meta-analysis. Archives of internal medicine. 2005; 165: 2337-2344.
- Hsieh WS, Lemas MV, Ambinder RF. The biology of Epstein-Barr virus in post-transplant lymphoproliferative disease. Transplant infectious disease : an official journal of the Transplantation Society. 1999; 1: 204-212.
- Katsura Y, Suzukawa K, Kojima H, Yoshida C, Shimizu S, et al. Cytotoxic T-cell lymphoma arising in Behçet disease. International journal of hematology. 2003; 77: 282-285.
- Harada K, Ohtsuru K, Nakayama K, Takagi S, Sugita Y, et al. [Intracranial primary malignant lymphoma following Behçet’s disease--case report]. No to shinkei = Brain and nerve. 1992; 44: 1029-1033.
- Sakane T, Takeno M, Suzuki N, Inaba G. Behçet’s disease. The New England journal of medicine. 1999; 341: 1284-1291.
- Gottschalk S, Rooney CM, Heslop HE. Post-transplant lymphoproliferative disorders. Annual review of medicine. 2005; 56: 29-44.
- Au WY, Ma ES, Choy C, Chung LP, Fung TK, et al. Therapy-related lymphomas in patients with autoimmune diseases after treatment with disease-modifying anti-rheumatic drugs. American journal of hematology. 2006; 81: 5-11.
- Sun A, Chang JG, Chu CT, Liu BY, Yuan JH, Chiang CP. Preliminary evidence for an association of Epstein-Barr virus with pre-ulcerative oral lesions in patients with recurrent aphthous ulcers or Behçet’s disease. Journal of oral pathology & medicine : official publication of the International Association of Oral Pathologists and the American Academy of Oral Pathology. 1998; 27: 168-175.
- Delecluse HJ, Feederle R, O’Sullivan B, Taniere P. Epstein Barr virus-associated tumours: an update for the attention of the working pathologist. Journal of clinical pathology. 2007; 60: 1358-1364.
- Feng YF, Wu QL, Zong YS. Correlation of immunophenotype of sinonasal non-Hodgkin’s lymphoma to Epstein-Barr virus infection. Chinese journal of cancer. 2007; 26: 1170-1176.