
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Squamous cell carcinoma of scrotum- A confounding entity amongst benign lesions: A case report
Priyanka Shinde1*; Venkatasubramanian R2; Muralidharan M3
1Senior Resident, Department of General surgery, Apollo Main hospitals, Chennai, Tamil Nadu, India.
2Consultant Laparoscopic Surgeon, Apollo Main hospitals, Chennai, Tamil Nadu, India.
3Director Medical Education, Southern region, Apollo Main hospitals, Chennai, Tamil Nadu, India.
*Corresponding Author : Priyanka Shinde
Kaushalya Hospital, Kulkarni baug lane 4, College Road, Nashik 422005, Maharashtra, India.
Tel: +919881965577;
Email: priyankashindep@gmail.com
Received : Feb 20, 2023
Accepted : Mar 09, 2023
Published : Mar 16, 2023
Archived : www.jcimcr.org
Copyright : © Shinde P (2023).
Abstract
Introduction: Squamous cell carcinoma of the scrotum is a rare entity, the current incidence being 1 per million males/year. It was among the first occupational malignancies identified.
Case report: A 45- year- old man with multiple sebaceous cysts of the scrotum, presented with a nodular ulcerated lesion over the right hemi-scrotum for 2 months, which appeared after incision and drainage of an abscess at the same site. On histological examination, it was found to be a well-differentiated squamous cell carcinoma. He was managed with wide local excision and primary closure of the skin defect. Post-operative recovery was uneventful.
Discussion: Although first reported as occupational in etiology, other causes such as HPV infection are now known to cause Scrotal carcinoma. The stage of the disease can influence the prognosis. This lesion can arise in a setting of other benign conditions like multiple sebaceous cysts, as in this case, often confounding the diagnosis. Hence a differential diagnosis of malignancy must be considered in all patients presenting with scrotal lesions.
Keywords: Squamous cell Carcinoma; Scrotum; Scrotal cancer.
Citation: Shinde P, Venkatasubramanian R, Muralidharan M. Squamous cell carcinoma of scrotum- A confounding entity amongst benign lesions: A case report. J Clin Images Med Case Rep. 2023; 4(3): 2327.
Introduction
Squamous cell carcinoma of the skin is the second most common skin cancer; however, squamous cell carcinoma arising from the scrotum is a rare entity, the current incidence being 1 per million males/year [1-4]. Sir Percivall Pott in the year 1775, was the first person to report an association between occupational exposure to soot in chimney sweepers in England and scrotal cancer, hence, is it also called as Chimney Sweep’s carcinoma [5]. The associated risk factors are exposure to tar, shale oil, paraffin oil pressing [4-8], with a recent shift towards iatrogenic phototherapy [1], PUVA exposure, HPV infection and chronic infection [9-11]. It usually presents as a scrotal nodule or a plaque [12]. It can uncommonly present as an ulcer, an abscess, developing in the scar of Fournier’s gangrene or an epidermal cyst, confounding the diagnosis [13-20]. We present a rare case of squamous cell carcinoma of scrotum along with multiple scrotal sebaceous cysts.
Case presentation
The patient was a 45-year- old male, who worked at a fuel pump and presented with a nodulo-ulcerated lesion over the right anterior hemi-scrotum for 2 months. He also had several sebaceous cysts of varying sizes all over the scrotum for the last 6 years.
He first noticed a swelling 6 months ago, which gradually increased in size, was painful and ruptured spontaneously with pus discharge. He visited a local hospital and an incision and drainage of the abscess with primary closure was performed. Thereafter, he noticed recurrence of the swelling at the same surgical site, which gradually increased in size over 2 months. There was no history of pain or pus discharge from the swelling.
His past history revealed multiple, asymptomatic sebaceous cysts of different sizes all over the scrotum, for 6 years.
Incidentally, he also suffered from chronic hepatitis B infection, hypertension, and Stage -V chronic kidney disease needing regular haemodialysis.
Clinical examination revealed a 4 x 2 cm well-defined, nodulo-ulcerated lesion over the right hemi-scrotum (Figure 1). It appeared to arise from the skin surface and was distinct from the underlying testis. The swelling was fleshy pink in colour, mobile, non-tender, with no local rise of temperature over the swelling. Rest of the scrotum had multiple mobile, non-tender, well defined, smooth surfaced swellings ranging from 1 x 1 cm up to 5 x 6 cm. The right and left testes, cord structures and penis were normal. There was no associated inguinal lymphadenopathy. General examination revealed mild ascites. Rest of the systemic examination was essentially normal. Routine biochemical and haematological investigations were normal. Ultrasound of the whole abdomen showed features of chronic liver disease, mild to moderate ascites with floating internal echoes; splenic enlargement, consistent with the history of chronic liver disease. There was no evidence of lymph node enlargement. Scrotal doppler showed features of multiple, well - defined isoechoic lesions in the scrotal wall with no internal vascularity or calcification.
The patient’s health was optimized before surgery, written consent was taken, wide local excision of the lesion with excision of multiple sebaceous cysts was done and the wound was closed primarily.
The histopathological examination revealed a well differentiated squamous cell carcinoma of the scrotal skin (Figure 2). The infiltrating neoplasm was composed of irregular nests of cells with pleomorphic vesicular nuclei, dyskeratosis and keratin pearls surrounded by fibrous stroma with subacute inflammation and increase mitosis (Figure 3). The resected margins were microscopically free from the tumour. He was deemed Lowe’s stage [11] A1 (Table 1).
The patient recovered uneventfully and was discharged on the second postoperative day. He was advised to follow-up with an Oncologist.

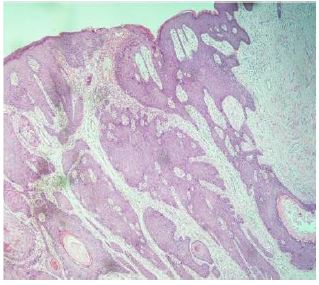
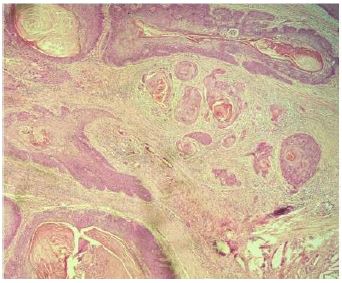
Table 1: Lowe’s staging for scrotal squamous cell carcinoma [11]. (adapted from Vyas R, Zargar H, Trolio RD, Di Lorenzo G, Autorino R. Squamous cell carcinoma of the scrotum: A look beyond the chimneystacks. World J Clin Cases. 2014; 2(11): 654-660).
| Stage | Description |
|---|---|
| A1 | Disease localised to scrotum. |
| A2 | Locally extensive disease involving adjacent structures (penis, perineum, testis or cord, and pubic bone) by continuity but without evident metastasis. |
| B | Superficial lymph node metastasis, resectable. |
| C | Pelvic lymph node metastasis, or any unresectable metastasis. |
| D | Distant metastasis beyond regional nodes. |
Discussion
Squamous cell carcinoma of the scrotum was the first occupational malignancy to be reported [5]. With the improvement of general health practices this disease has become rare in the modern world with the current incidence being 1 per million males/year [1-4].
Exposure to tar, shale oil, paraffin oil pressing, poor hygiene, chronic inflammation, immunosuppression, PUVA therapy, HPV infection and radiation exposure have all been linked to the development of scrotal cancers [4-11,21,22]. In current literature, occupation is no longer an etiological factor for squamous cell carcinoma but rather comorbidities, lifestyle, or HPV infections are associated with it [4,10,21,22]. Basaloid and warty subtypes are the most common histological subtypes of squamous cell carcinoma associated with high-risk HPV 16/18 infections [10,21,22]. However, in our patient, his chronic renal failure could be a potential predisposing factor to squamous cell carcinoma as mentioned in the study done by Matoso et al [10,23].
Primary scrotal carcinomas usually present as solitary, slow growing lesions or ulcers, which are limited to one hemi-scrotum, mostly over the anterior- inferior aspect with or without regional lymph node involvement [16]. Their histological subtypes include squamous cell carcinoma, extramammary Paget’s disease, sarcoma, basal cell carcinoma, melanoma, and adnexal tumours, with squamous cell carcinoma having the greatest propensity for regional lymph node metastasis [4,11,23]. The histopathological variants of cutaneous squamous cell carcinoma include verrucous, spindle, desmoplastic, and acantholytic types. Amongst these, the desmoplastic variant is characterized by highly infiltrative growth, with a large amount of stroma and narrow cord of cells, whereas the acantholytic variant is characterized by intramural pseudo-glandular structures and both are associated with a high risk of lymph node metastasis [24].
Significant predictors of survival are the age of the patient, stage of the disease as given by Lowe staging and histological grade of the tumour; hence, a high index of suspicion is necessary to make an early diagnosis [7,8,11]. The treatment of choice is surgery in the form of wide local excision to achieve a negative margin [11,12]. The wound can be closed primarily, large defects are amenable to plastic surgery reconstruction. Inguinal lymph node dissection may be performed in clinically enlarged and biopsy proven high risk cases; however, prophylactic lymph node dissection is not recommended [11,20]. Neo-adjuvant therapy can be used to downstage the disease [24]. Adjuvant chemotherapy using a combination of bleomycin, cisplatin, and methotrexate can be used for operable as well as metastatic or inoperable disease [25,26]. Targeted therapy might hold some promise in the near future for advanced squamous cell carcinomas [27].
Conclusion
Through this case we would like to throw light on one of the myriad of presentations of squamous cell carcinoma of the scrotum amongst benign conditions like scrotal abscess, nodules, ulcers, epidermal cysts, chronic scars, Marjolin’s ulcer and Fournier’s gangrene, thus, confounding the surgeon. Hence, a differential diagnosis of squamous cell carcinoma scrotum must be kept in mind whilst evaluating any patient presenting with a scrotal lesion.
Declarations
Conflict of interest: None declared.
Patient consent: Written informed consent was obtained from the patient for publication of this case report.
Statement of ethics: Approval was taken from The Institutional Ethics Committee- Bio Medical Research, Apollo Hospitals, Chennai, Tamil Nadu, India.
Funding: No funding for received for the preparation of this manuscript.
References
- Howell JY, Ramsey ML. Squamous Cell Skin Cancer. [Updated 2021 Aug 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2022.
- Verhoeven RH, Louwman WJ, Koldewijn EL, Demeyere TB, Coebergh JW. Scrotal cancer: incidence, survival and second primary tumours in the Netherlands since 1989. Br J Cancer. 2010; 103: 1462-1466.
- Wright JL, Morgan TM, Lin DW. Primary scrotal cancer: disease characteristics and increasing incidence. Urology. 2008; 72: 1139-1143.
- Sarkar D. A systematic review of scrotal squamous cell carcinoma. EMJ Urol. 2019; 7: 68-74.
- Kipling MD, Waldron HA. Percivall Pott and cancer scroti. Br J Ind Med. 1975; 32: 244-246.
- Verhoeven RH, Kiemeney LALM, Coebergh JWW, Weiderpass E, Kjaerheim K, et al. Occupation and scrotal cancer: Results of the NOCCA study. Acta Oncol. 2011; 50: 1244-1246.
- Johnson TV, Hsiao W, Delman KA, Canter DJ, Master VA, et al. Scrotal cancer survival is influenced by histology: A SEER study. World J Urol. 2013; 31: 585-590.
- Fay HT. Risk factors in scrotal epithelioma. J R Soc Med. 1978; 71: 741-747.
- Stern RS, Bagheri S, Nichols K. The persistent risk of genital tumors among men treated with psoralen plus ultraviolet A (PUVA) for psoriasis. J Am Acad Dermatol. 2002; 47: 33-39.
- Matoso A, Ross HM, Chen S, Allbritton J, Epstein JI. Squamous neoplasia of the scrotum: a series of 29 cases. Am J Surg Pathol. 2014; 38: 973-981.
- Vyas R, Zargar H, Trolio RD, Di Lorenzo G, Autorino R. Squamous cell carcinoma of the scrotum: A look beyond the chimneystacks. World J Clin Cases. 2014; 2: 654-660.
- McDonald MW. Carcinoma of scrotum. Urology. 1982; 19: 269-274.
- Huen KH, Nourparvar P, Decaro JJ, Walsh MD, Issa MM, Ritenour CW. Scrotal abscess as initial presentation of squamous cell carcinoma. Case Rep Urol. 2013; 2013: 807346.
- Garzon R, Burgos EB, Garzon FL, Cippitelli L, de Cabalier ED, Cabalier LR. Marjolin ulcer. Rev Fac Cien Med Univ Nac Cordoba. 2001; 58: 93-97.
- Sabin SR, Goldstein G, Rosenthal HG, Haynes KK. Aggressive squamous cell carcinoma originating as a Marjolin’s ulcer. Dermatol Surg. 2004; 30: 229-230.
- Chintamani, Shankar M, Singhal V, Singh JP, Bansal A, Saxena S. Squamous cell carcinoma developing in the scar of Fournier’s gangrene-case report. BMC Cancer. 2004; 4: 16.
- Abdalla Saad Abdalla Al-Zawi, Sadaf Memon, Ahmed Shah, Soad Eldruki, Elizabeth Tan, Salem Omar Alowami. A squamous cell carcinoma arising from scrotal epidermal cyst. A case report and review of 94 cases from the world literature. Journal of Oncology. 2019; 69: 150-156.
- Lun-Pin Yeh, Kuo-Sheng Liao. Squamous cell carcinoma arising from an epidermal cyst of the scrotum. Tzu Chi Medical Journal. 2013; 25: 117-118.
- Schneider PR, Russell RC, Zoo EG. Fournier’s gangrene of the penis: a report of two cases. Ann Plast Surg. 1986; 17: 87-90.
- Yumura Y, Chiba K, Saito K, Hirokawa M. Fournier’s gangrene in a patient with malignant lymphoma: a case report. Hinyokika Kiyo. 2000; 46: 735-737
- Matoso A, Fabre V, Quddus MR, Lepe M, Lombardo KA, et al. Prevalence and distribution of 15 high-risk human papillomavirus types in squamous cell carcinoma of the scrotum. Hum Pathol. 2016; 53: 130-136.
- Andrews PE, Farrow GM, Oesterling JE. Squamous cell carcinoma of the scrotum: long-term followup of 14 patients. J Urol. 1991; 146: 1299-1304.
- Stratigos A, Garbe C, Lebbe C, Malvehy J, del Marmol V, Pehamberger H, Peris K, Becker JC, Zalaudek I, Saiag P, Middleton MR, Bastholt L, Testori A, Grob JJ; European Dermatology Forum (EDF); European Association of Dermato-Oncology (EADO); European Organization for Research and Treatment of Cancer (EORTC). Diagnosis and treatment of invasive squamous cell carcinoma of the skin: European consensus-based interdisciplinary guideline. Eur J Cancer. 2015; 51: 1989-2007.
- Motley R, Kersey P, Lawrence C; British Association of Dermatologists; British Association of Plastic Surgeons. Multiprofessional guidelines for the management of the patient with primary cutaneous squamous cell carcinoma. Br J Plast Surg. 2003; 56: 85-91.
- Arai Y, Kinouchi T, Kuroda M, Usami M, Kotake T. A case of scrotal cancer with inguinal lymph node metastasis treated by multidisciplinary modalities including chemotherapy with methotrexate, bleomycin and cisplatin. Hinyokika Kiyo. 1997; 43: 683-685.
- Dexeus FH, Logothetis CJ, Sella A, Amato R, Kilbourn R, Fitz K, et al. Combination chemotherapy with methotrexate, bleomycin and cisplatin for advanced squamous cell carcinoma of the male genital tract. J Urol. 1991; 146: 1284-1287.
- Carthon BC, Ng CS, Pettaway CA, Pagliaro LC. Epidermal growth factor receptor-targeted therapy in locally advanced or metastatic squamous cell carcinoma of the penis. BJU Int. 2014; 113: 871-877.