
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A case report of tracheobronchopathia osteochondroplastica
Qian Li; Juan Huang; Wenli Wang*
Department of General Medicine, Chongqing general hospital, China.
*Corresponding Author : Wenli Wang
Department of General Medicine, Chongqing General Hospital, China.
Email: 476223464@qq.com
Received : Feb 22, 2023
Accepted : Mar 10, 2023
Published : Mar 17, 2023
Archived : www.jcimcr.org
Copyright : © Wang W (2023).
Abstract
Background: Tracheobronchopathia Osteochondroplastica (TO) is a benign disease of low incidence that is characterized by multiple submucosal cartilaginous and bony tracheobronchial nodules. There is still no unified standard or guideline for the diagnosis and treatment of TO worldwide. This case report may help reduce clinical misdiagnosis and missed diagnosis while providing accurate diagnosis and treatment for this disease.
Case presentation: We report a 58-year-old man who had a history of coughing and sore throat for one month and was finally diagnosed with TO. In this case, we identified the typical features of TO by imaging, bronchoscopy, and pathological biopsy.
Conclusion: The diagnosis of TO mainly relies on imaging, bronchoscopy and pathological biopsy. There is no specific drug that can treat TO. For asymptomatic or mild symptoms, no special treatment is needed. When the central airway lumen is severely narrowed, bronchoscopy or surgical resection is required.
Keywords: Tracheobronchial osteochondroplastica; Tracheobronchopathia osteoplastica; Tracheobronchopathia osteochondroplastica.
Abbreviations: TO: Tracheobronchopathia Osteochondroplastica; CRP: C-Reactive Protein; PCT: Procalcitonin; ESR: Erythrocyte Sedimentation Rate; ANCA: Antineutrophil Cytoplasmic Antibody; AFP: Alpha Fetoprotein; CEA: Carcinoembryonic Antigen; CA50: Carbohydrate Antigen 50; CA199: Carbohydrate Antigen 199; CA125: Carbohydrate Antigen 125; SFE: Serum Ferritin; PPD: Tuberculin Pure Protein Derivative Test; CT: Computed Tomography; GM: Galactomannan; TBA: Tracheobronchial Amyloidosis; BMP-2: Bone Morphogenetic Protein 2; TGF-Beta 1: Transforming Growth Factor Beta-1.
Citation: Li Q, Huang J, Wang W. A case report of tracheobronchopathia osteochondroplastica. J Clin Images Med Case Rep. 2023; 4(3): 2330.
Background
Tracheobronchopathia osteochondroplastica (TO) is a rare benign disease affecting the lumen of the tracheobronchial tree. Multiple submucosal cartilaginous and bony tracheobronchial nodules are observed characteristically in TO [1]. TO was first described in 1857 as ossific deposits in the larynx, trachea and bronchi. The accumulation of calcium phosphate in the submucosa of large airways and benign proliferation of bone and cartilage lead to narrowing of the airways [1]. Furthermore, the cytokines BMP-2 and TGF-beta 1 are also involved in inducing new bone formation during the progression of TO [2]. There is still no unified standard or guideline for the diagnosis and treatment of TO worldwide. In this case, we analysed the diagnostic process for this uncommon disease, and this report might provide a potential reference for the clinical diagnosis and treatment of similar cases.
Case presentation
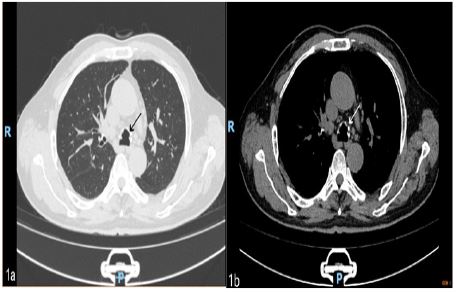
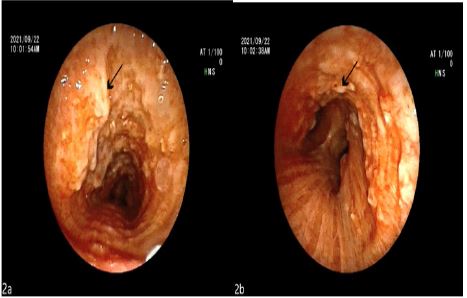
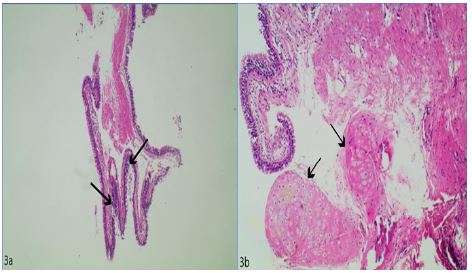
A 58-year-old male was admitted to the hospital with increased blood glucose levels lasting longer than 1 month. His medical history mainly included high blood sugar, continuous coughing and sore throat without clear aetiology, excluding dyspnoea, haemoptysis, hoarseness, wheezing, hot flashes occurring in the afternoon and night sweats. The patient denied a history of chronic bronchitis and tuberculosis, smoking, and allergies. He was diagnosed with tonsilitis in another hospital and did not improve after taking azithromycin for more than 10 days. The physical examination showed that the whole-body lymph nodes were not palpable or enlarged, the bilateral tonsils were classified as Grade 1, there was no purulent secretion on the surface, the pharynx was slightly congested, the lungs were clear and symmetrical, and no dry or wet rales were heard. Auxiliary examination showed that routine blood, CRP, PCT, liver function, renal function, electrolytes, coagulation, ESR, ANCA, antinuclear antibody spectrum, AFP, CEA, CA50, CA199, CA125, SFE, and thyroid function tests all reported negative results. A PPD skin test was positive. Chest CT scan showed extensive calcification of the trachea and bronchi in the upper lobes of the lungs with inflammation and atelectasis in the lower lobes of the lungs. Fibreoptic bronchoscopy showed nodular protrusions of different sizes in the trachea and bronchial mucosatracheobronchial inflammation changes. Simultaneous detection of multiple respiratory pathogens in the alveolar lavage fluid yielded positive results for Streptococcus pneumoniae, Klebsiella pneumoniae, and Pseudomonas aeruginosa; weak positive results for mycobacterium tuberculosis complex, human herpes virus type 4, and human herpes virus type 7; and negative results for fungi, mycoplasma and chlamydia. Alveolar lavage fluid culture results were positive for Pseudomonas aeruginosa and Klebsiella pneumoniae. Pathological examination of alveolar lavage fluid revealed a small number of inflammatory cells. The acid-fast bacillus test, GM test, and tuberculosis fast culture of alveolar lavage fluid reported negative results. Pathological examination of nodules on the inner wall of the trachea revealed chronic inflammation of the mucosa with epithelial hyperplasia, and bronchial cartilage was seen locally. Final diagnosis considerations included secondary pulmonary tuberculosis, smear (-) gene (+) culture (-) initial treatment, and tracheobronchopathia osteochondroplastica.
Discussion
The most frequent manifestation in TO is chronic cough; other symptoms include sputum, dyspnoea on exertion, haemoptysis, chest tightness and pain, continuous or intermittent fever, dryness of the throat, and hoarseness, even in the early stage of the disease, which can be asymptomatic. Therefore, misdiagnosis and missed diagnosis of TO are very common [3]. TO is primarily discovered accidentally in the clinic, and more than 90% of cases are diagnosed by further examination. The cause of TO remains unknown. Some studies have reported that the aetiology of TO may be related to chronic infection, congenital abnormalities, chemical or mechanical stimulation, degenerative or metabolic abnormalities, genetic predispositions or chronic inflammation [4]. Among these, chronic inflammation was thought to be the most relevant factor in the course of TO. Studies have also confirmed that localized TBA may be the cause of TO [5]. In our case, the patient had chronic coughing and sore throat and did not improve after taking antibiotics. He has been engaged in home decoration for many years; long-term exposure to dust and certain odours and chronic infections caused by secondary tuberculosis may be the cause.
The diagnosis of TO mainly relies on CT, bronchoscopy and histopathological examination. Chest CT scans typically show extensive calcification of the trachea and bronchi, with calcified nodules protruding into the tracheobronchial lumen. Bronchoscopy is the gold standard for TO diagnosis [6,7]. The incidence rate of TO diagnosis during autopsy is 1/6000~48/6000, and the incidence rate using bronchoscopy is 2.5/1000~3/1000 [8-11]. A large cohort study in China divided TO into three stages based on bronchoscopy and histopathology. In stage I (early, mild), chondrocytes are occasionally seen, and bronchoscopy shows scattered yellow-white soft plaque lesions infiltrating the lumen and covering the lumen mucosa. In stage II (medium, moderate), sessile spicules and cartilaginous nodules can be seen, and bronchoscopy shows cobblestone or stalactite cave-like changes in the cavity. In stage III (late, severe), flaky bone and fatty bone marrow accompanied by haematopoietic formation can be seen, and bronchoscopy shows that the tracheal wall is deformed and stiff, and the airway is narrowed or even blocked [12]. Submucosal biopsy is necessary to diagnose and distinguish other airway diseases, such as tracheobronchial amyloidosis, atrophic chondritis, tracheobronchiopapillomatosis, tracheobronchial calcinosis, granulomatous diseases such as tuberculosis and sarcoidosis, and malignant tumours [13-16]. According to the bronchoscopy results, the patient in this case was diagnosed as stage II. Submucosal biopsy revealed chronic inflammation of the mucosa with epithelial hyperplasia, and bronchial cartilage was visible at the focal point. The diagnosis was finally confirmed. This patient was unique because TO was associated with secondary tuberculosis. If the alveolar lavage fluid is not tested for pathogens, there may be a missed diagnosis.
There is no specific drug that can treat TO. According to the patient’s symptoms and the severity of airway obstruction, TO treatment methods include symptomatic treatment, cryotherapy, laser treatment, bronchoscopy intervention, surgical resection, and radiotherapy [17,18]. Since most TPOs progress slowly, conservative treatment is usually sufficient [14,19]. For asymptomatic or mild symptoms, no special treatment is needed. Studies have shown that inhaled corticosteroids may be useful for lesions comprised of inflammatory cells and cartilaginous nodules but may have little effect on lesions comprised of osteocytes and lamellar bone, so they may be useful for most patients with stage I and II disease. For patients with stage II or III disease, the effect of inhaled corticosteroids on TO is minimal. In addition, the effective dosage and treatment duration with the fewest side effects need to be studied further [12]. When the central airway lumen is severely narrowed, bronchoscopy or surgical resection is necessary. Our patient’s condition was more complicated. During hospitalization, due to diabetes, poor blood sugar control and secondary tuberculosis, inhaled corticosteroids were not used, so their efficacy could not be observed. Levofloxacin 0.5 g was administered intravenously once a day for anti-infective treatment, and the anti-tuberculosis quadruple drug treatment duration was short, so no curative effect was observed. The patient was followed up after discharge. He insisted on taking anti-tuberculosis drugs and did not take any other medication. His cough and sore throat were relieved, and the patient was satisfied with this result. Therefore, it is uncertain whether cough and sore throat are related to TO. Long-term follow-up is still required in the later stages.
Declarations
Ethics approval and consent to participate: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Consent for publication: Written informed consent for publication was obtained from the participant.
Availability of data and materials: Not applicable.
Competing interests: The authors declare that they have no competing interests.
Funding: Not applicable.
Authors’ contributions: QL was responsible for the literature review, design, and writing of the manuscript. JH and WW participated in the diagnosis and treatment, and revised the manuscript. All authors read and approved the final manuscript.
Acknowledgements: Not applicable.
References
- Lazor R, Cordier JF. Tracheobronchopathia osteochondroplastica.Orphanet Encyclopedia. 2004; 1-4.
- Tajima K, Yamakawa M, Katagiri T. Immunohistochemical detection of bone morphogenetic protein-2 and transforming growth factor beta-1 in tracheopathia osteochondroplastica. Virchows Arch. 1997; 431: 359-363.
- Li DD, Jin FG, Nan YD, Jiang H, Liu Q, et al. Multi-nodule of large airway: tracheobronchopathia osteochondroplastica. Ann Palliat Med. 2021; 10: 1115-1121.
- Doshi H, Thankachen R, Philip MA, Kurien S, Shukla V, Korula RJ. Tracheobronchopathia osteochondroplastica presenting as an isolated nodule in the right upper lobe bronchus with upper lobe collapse. J Thorac Cardiovasc Surg. 2005; 130: 901-902.
- Song JY, Kim BG, Zo S, Park S, Han JH, et al. Tracheobronchopathia osteochondroplastica (TPO) associated with tracheobronchial amyloidosis (TBA). Respir Med Case Rep.2020; 31: 101158.
- Li YY, Hu CP, Yang HZ, Yang HP, Qu SJ, et al. The diagnostic value of flexible bronchoscopy in tracheobronchopathia osteochondroplastica[J]. Zhonghua Jie He He Hu Xi Za Zhi. 2009; 32: 489-492.
- Abu-Hijleh M, Lee D, Braman SS. Tracheobronchopathia osteochondroplastica: a rare large airway disorder. Lung. 2008; 186: 353-359.
- Prakash UB. Tracheobronchopathia osteochondroplastica. Semin Respir Crit Care Med. 2002; 23: 167-175.
- Tatar D, Senol G, Demir A, Polat G. Tracheobronchopathia osteochondroplastica: four cases. Chin Med J (Engl). 2012; 125: 2942-2944.
- Jabbardarjani HR, Radpey B,Kharabian S, Masjedi MR. Tracheobronchopathia osteochondroplastica: presentation of ten cases and review of the literature. Lung. 2008; 186: 293-297.
- Perez-Rodriguez E, Nunez N, Alvarado C, Golpe A, Casanova C, et al. Diagnosis of Tracheobronchopathia osteochondroplastica. Chest. 1990; 97: 763.
- Zhu Y,Wu N, Huang HD, Dong YC, Sun QY, et al. A clinical study of tracheobronchopathia osteochondroplastica: findings from a large Chinese cohort. PLoS One. 2014; 9: e102068.
- Chrysikos S, Karampitsakos T, Tzouvelekis A, Dimakou K. Coexistence of tracheobronchopathia osteochondroplastica and sarcoidosis: accidental finding or something more?. J Bronchology Interv Pulmonol. 2019; 26: e7-e8.
- Ulasli SS, Kupeli E. Tracheobronchopathia osteochondroplastica: a review of the literature. Clin Respir J. 2015; 9: 386-391.
- Chroneou A, Zias N, Gonzalez AV, Beamis JF. Tracheobronchopathia osteochondroplastica. An underrecognized entity? Monaldi Arch Chest Dis. 2008; 69: 65-69.
- Zaibi H, Fessi R, Dhahri B, Ben Amar J, Aouina H. Tracheobronchopathia osteochondroplastica: end stage of tracheo-bronchial amyloidosis. Tanaffos. 2019; 18: 272-275.
- Wong JS, Ng CS, Yim AP. Hemoptysis with multiple tracheal nodules. Chest. 2005; 128: 3671-3673.
- Wang N, Long F, Jiang S. Tracheobronchopathia osteochondroplastica: two cases reports and review of literature. Medicine (Baltimore). 2016; 95: e3396.
- Hussain K, Gilbert S. Tracheopathia osteochondroplastica. Clin Med Res. 2003; 1: 239-242.