
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Spindle cell sarcoma of the heart and severe coronary artery disease following successfully treated colon cancer
Azin Alizadehasl1,4; Alia Bahramnejad1*; Amir Dousti2; Koorosh Kalantari2; Kamran Roudini3; Ronak Ahmadi4; Maryam Norouzi4
1Cardio-Oncology Research Center, Rajaie Cardiovascular Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran.
2Interventional Cardiology Research Center, Rajaie Cardiovascular Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran.
3Cancer Institute, Imam Khomeini Hospital, Tehran University of Medical Sciences, Tehran, Iran.
44Echocardiography Research Center, Rajaie Cardiovascular Medical and Research Center, Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Alia Bahramnejad
Rajaie Cardiovascular Medical and Research Center, Niayesh highway, Tehran, Iran.
Tel: +98-912-157-0518;
Email: Aaly_brnj@yahoo.com
Received : Feb 27, 2023
Accepted : Mar 13, 2023
Published : Mar 20, 2023
Archived : www.jcimcr.org
Copyright : © Bahramnejad A (2023).
Abstract
Spindle cell sarcoma (SCS) of the heart is a rare tumor which has malignant course, that could be primary tumor or metastasis. Chronic inflammation following cancer has a strong role in accelerated atherosclerosis and incidence of second cancer. Here we present a case of SCS and CAD following colon adenocarcinoma.
Keywords: Cancer; Acute coronary syndrome; Coronary angiography.
Abbreviations: LM: Left Main; VT: Ventricular Tachycardia; PTE: Pulmonary Thromboembolism; ECG: Electrocardiography; LV: Left Ventricle; LA: Left Atrium; RA: Right Atrium; RV: Right Ventricle; EF: Ejection Fraction; MR: Mitral Regurgitation; TR: Tricuspid Regurgitation; MV: Mitral valve; TV: Tricuspid Valve; TRG: Tricuspid Regurgitation Gradient; SPAP: Systolic Pulmonary Artery Pressure; IVC: Inferior Vena Cava; CT: Computed Tomography; LPA: Left Pulmonary Artery; MPA: Main Pulmonary Artery; LUPV: Left Upper Pulmonary Vein; IV: Intra Venous; CMR: Cardiac Magnetic Resonance; PCI: Percutaneous Coronary Intervention; NSTEMI: Non ST Elevation Myocardial Infarction; CABGS: Coronary Arteries Bypass Grafts Surgery; LVAD: Left Ventricle Assist Device; TTE: Trans Thoracic Echocardiography; TEE: Trans Esophageal Echocardiography; SCS: Spindle Cell Sarcoma; CAD: Coronary Artery Disease;
Citation: Alizadehasl A, Bahramnejad A, Dousti A, Kalantari K, Roudini K, et al. Spindle cell sarcoma of the heart and severe coronary artery disease following successfully treated colon cancer. J Clin Images Med Case Rep. 2023; 4(3): 2331.
Introduction
The most common cardiac tumors are metastatic ones, with the most prevalent sources from breast, lung and melanoma origins as solid tumors and hematologic malignancies like lymphoma as well [1]. The most common primary cardiac tumor is myxoma which is considered as a benign tumor but the most common primary malignant cardiac tumors are sarcomas [2]. Tumor like masses like thrombus and Lamble’s excrescences also should be considered [3]. Primary Spindle cell sarcoma of the heart is a very rare tumor which has malignant course with very poor prognosis [4]. Chronic inflammation following cancer has a strong role in accelerated atherosclerosis and incidence of second cancer [5]. We want to present a case of pericardial spindle cell sarcoma in a 61-year-old lady as a second cancer following treated colon cancer three years earlier. Finally, the patient succumbed because of Left Main (LM) and diffuse coronary artery disease and Ventricular Tachy-Arrhythmia (VT) storm.
Case presentation
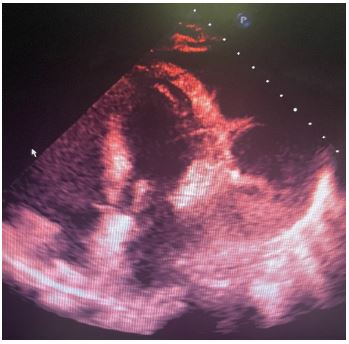
A 61-year-old lady with history of Colon adenocarcinoma in year 2019 which was treated by right Hemi-colectomy followed by chemotherapy and had no evidence of recurrence since 2022 and no major coronary artery disease risk factor. Six months before referring to our hospital she had Pulmonary Thromboembolism (PTE) which treated by DOACs but the shortness of breath continued and even became worse accompanied by cough, malaise and fatigue. In our hospital, Electrocardiography (ECG) showed normal sinus rhythm with no ST-T abnormality, the echocardiography showed Huge circumferential intra-pericardial mass with mixed effusion extended from Left Ventricle (LV) apex to Left Atrium (LA) with compressive effect on left heart structures (Figure 1); other echo findings included normal LV size with LV Ejection Fraction (EF): 50-55%, mildly enlarged Right Ventricle (RV) size with mildly reduced RV systolic function, normal LA and Right Atrium (RA) size, normal mitral and aortic valve appearance with mild mitral regurgitation (MR) and moderate to severe Tricuspid Valve Regurgitation (TR), exaggerated respiratory variation in mitral inflow (32%) but no significant respiratory variation in Tricuspid Valve (TV) inflow, Tricuspid Regurgitation Gradient (TRG): 80 mmHg, Systolic Pulmonary Artery Pressure (SPAP): 85 mmHg, normal inferior Vena cava (IVC) size and respiratory collapse.
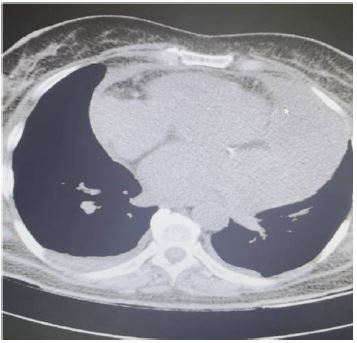
The patient underwent multi-slice spiral Computed Tomography (CT) scan of the thorax without contrast medium which showed large tumor in the pericardial space and invasion into the Left Pulmonary Artery (LPA), Main Pulmonary Artery (MPA), Left Upper Pulmonary Vein (LUPV) in favor of malignant tumor (Figure 2); also, CT scan denoted multiple tumors in left lung that the largest measured 18 mm and 20 x 8 mm suggestive for metastasis.
Multi-slice spiral CT scan of abdominal and Pelvic cavity without Intra-Venous (IV) contrast media revealed no evidence of colon cancer recurrence nor metastasis.
Cardio-Vascular Magnetic Resonance (CMR) with mass protocol showed normal cardiac chambers, volume and function.
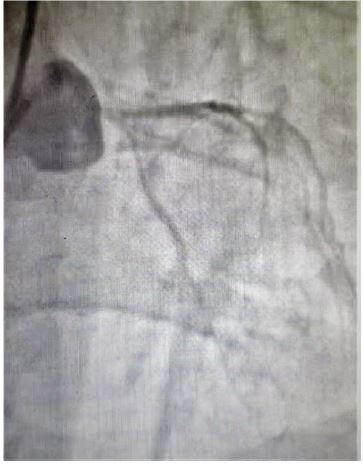
The patient underwent CT guided biopsy from the mass and discharged to wait for pathology report which showed inadequate tissue. Meanwhile she came to emergency department with signs and symptoms of pulmonary edema; in primary evaluations she had diffuse ST segment depression in ECG and echocardiography showed decreased LVEF to 30% and level of serum Troponin was high, so the patient with diagnosis of non ST elevation myocardial infarction (NSTEMI) and acute heart failure underwent coronary angiography which showed subtotal cut off of left main (LM) coronary artery with faint distal run off and diffuse coronary artery disease (Figure 3) which once tried to wire it for percutaneous coronary intervention (PCI) but exactly after wiring severe hypo-tension occurred which banned the interventional cardiologist to continue the procedure.
Consult to cardiac surgeon was done for tumor extraction and also Coronary Artery Bypass Graft Surgery (CABGS) but the cardiac surgeon refused surgery due to high-risk situation and extension of tumor invasion; with consideration of not having pathology, unstable hemodynamics, and refractory chest pain, it was impossible to start neo-adjuvant chemo-therapy. Therefore another CT guided biopsy was done which later reported spindle cell sarcoma.
Unfortunately, in course of hospitalization before having the report of pathology, the patient had refractory chest pain and was planned to retry for PCI with support of LV assist device (LVAD) but before performing of this plan she succumbed because of frequent and refractory ventricular tachy-arrhythmia (VT) despite administering of IV anti-arrhythmia medications such as Amiodarone and lidocaine.
Discussion
Spindle cell sarcoma of the heart is a very rare tumor which could be primary tumor of the heart or could be a primary lung cancer that metastases to the heart [6]. Spindle cell sarcoma may involve different structures of the heart such as left and right atrium, pulmonary veins, and pericardium [7]. There are many diagnostic modalities for cardiac masses that one covers weakness of other such as Trans-Thoracic Echocardiography (TTE), Trans-Esophageal Echocardiography (TEE), CT scan, and CMR, but early diagnosis of cardiac tumor is limited by lack of early symptoms and also, early treatment is limited by histopathology, location, and extension of Tumor [8]. Surgical resection is the main treatment for cardiac sarcomas and also some types of cardiac sarcomas may respond to chemotherapy [4].
There is a relationship between cancer and atherosclerosis, increased life expectancy of patients with both diseases, led to have patients with concomitant cancer and atherosclerosis, which may be related to common risk factors and medications [9]. Chronic inflammation in patients with cancer is linked to development of accelerated atherosclerosis and also second cancer [10]. There are Similar molecular pathways in pathogenesis and progression of these two diseases such as oxidative stress and cellular damage [1].
Sanjay Mehra et al described a case of spindle cell sarcoma of the heart in a 46-year-old female who underwent thoracotomy but considered inoperable due to extension of tumor and the patient expired after the surgery [4].
Paul Lajos et al reported a case of spindle cell sarcoma of pericardium which was inoperable due to invasion to mediastinal structures but after three cycles of neo-adjuvant therapy with ifosfamide, doxorubicin, and mesran, significant reduction of tumor invasion occurred and the patient underwent operation and was discharged six days after surgery [6].
Joo Hyun Park et al described a case of pericardial spindle cell sarcoma which at first misdiagnosed as a left main coronary artery disease but then thanks to coronary CT angiography, diagnosed as compression effect of tumor and successfully treated by surgical resection and CABGS [7].
Conclusion
Spindle cell carcinoma of the heart is a very rare tumor with poor prognosis but can be treated by surgery and neo-adjuvant therapy. Accelerated atherosclerosis may occur in patients with cancer which may result in mortality.
Declarations
Disclosure: The authors have nothing to disclose.
Funding: There was no funding.
References
- Zakhartseva LM, Zakharova LP, Shatrova KM, Chitaeva GE, Vitovsky RM. METASTATIC CARDIAC TUMORS: LITERATURE REVIEW AND OWN OBSERVATION OF TESTICULAR TUMOR METASTASIS IN THE RIGHT VENTRICLE OF THE HEART. Experimental Oncology. 2018; 40: 336-342.Zakhartseva LM, Zakharova LP, Shatrova KM, Chitaeva GE, Vitovsky RM. METASTATIC CARDIAC TUMORS: LITERATURE REVIEW AND OWN OBSERVATION OF TESTICULAR TUMOR METASTASIS IN THE RIGHT VENTRICLE OF THE HEART. Experimental Oncology. 2018; 40: 336-342.
- Bussani R, Castrichini M, Restivo L, Fabris E, Porcari A, Ferro F, et al. Cardiac Tumors: Diagnosis, Prognosis, and Treatment. Current Cardiology Reports. 2020; 22.
- Tyebally S, Chen D, Bhattacharyya S, Mughrabi A, Hussain Z, et al. Cardiac Tumors. J Am Coll Cardiol CardioOnc. 2020; 2: 293-311.
- Mehra S, Ibrahim O, Moshiri M, Cahill J, Bhargava P. Spindle-cell sarcoma of the heart: A rare cause for a cardiac mass. Radiology case reports. 2012; 7: 792.
- Hasselbalch HC. Perspectives on chronic inflammation in essential thrombocythemia, polycythemia vera, and myelofibrosis: is chronic inflammation a trigger and driver of clonal evolution and development of accelerated atherosclerosis and second cancer?. Blood, The Journal of the American Society of Hematology. 2012; 119: 3219-3225.
- Lajos P, Choo E, Hasaniya N, Ehrman W, Razzouk A. Spindle cell sarcoma of the pericardium: A case report. Journal of Cardiac Surgery. 2004; 19: 139-141.
- Park JH, Choe H, Jang WI, Hur G. Primary pericardial spindle cell sarcoma mimicking left main coronary artery disease. European journal of cardio-thoracic surgery. 2012; 41: 1179-1181.
- Mehra S, Ibrahim O, Moshiri M, Cahill J, Bhargava P. Spindle-cell sarcoma of the heart: A rare cause for a cardiac mass. Radiology case reports. 2012; 7: 792.
- Raposeiras Roubı´n S, Cordero A. The two-way relationship between cancer and atherosclerosis. Rev Esp Cardiol. 2019.
- Hasselbalch HC. Perspectives on chronic inflammation in essential thrombocythemia, polycythemia vera, and myelofibrosis: is chronic inflammation a trigger and driver of clonal evolution and development of accelerated atherosclerosis and second cancer?. Blood, The Journal of the American Society of Hematology. 2012; 119: 3219-3225.
- Ross JS, Stagliano NE, Donovan MJ, Breitbart RE, Ginsburg GS. Atherosclerosis and cancer: common molecular pathways of disease development and progression. Annals of the New York Academy of Sciences. 2001; 947: 271-93.