
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
A case of rhino-orbital cerebral mucormycosis presenting with
spontaneous cerebrospinal fluid rhinorrhoea
Rajesh Verma*; Rajarshi Chakraborty; Keerthiraj DB
Department of Neurology, King George’s Medical University, Lucknow, India.
*Corresponding Author : Rajesh Verma
Department of Neurology, King George’s Medical University, Lucknow, India.
Tel: 09335915823;
Email: drrajeshverma32@yahoo.com
Received : Feb 25, 2023
Accepted : Mar 13, 2023
Published : Mar 20, 2023
Archived : www.jcimcr.org
Copyright : © Verma R (2023).
Abstract
Rhino-orbital cerebral mucormycosis has increased in the recent second wave of post-COVID-19 illness, mainly in tropical countries like India. The burden of diabetes mellitus and rampant use of corticosteroid, environmental factors, post-COVID-19 immunological derangement might be contributory factors to the development of extensive outbreak of ROCM. Cerebrospinal fluid rhinorrhea is rarely documented with such fungal infection in literature. This case report described a 45-year diabetic woman in the post-COVID-19 phase,who developed rhino-orbital cerebral mucormycosis, presenting with spontaneous cerebrospinal fluid rhinorrhea.
Keywords: Mucormycosis; Cerebrospinal fluid; Post-covid-19 phase; Corticosteroid; Orbital exenteration.
Keymessage: Rhino-orbital cerebral mucormycosis has increased in the recent second wave of the post-COVID-19 phase. The burden of diabetes mellitus and rampant use of corticosteroids, environmental factors, post-COVID-19 immunological derangement might contribute to the endemic of ROCM. Cerebrospinal fluid rhinorrhea is rarely documented with such fungal infection in literature.
Citation: Verma R, Chakraborty R, Keerthiraj DB. A case of rhino-orbital cerebral mucormycosis presenting with spontaneous cerebrospinal fluid rhinorrhoea. J Clin Images Med Case Rep. 2023; 4(3): 2332.
Introduction
Rhinorbital Cerebral Mucormycosis (ROCM) is an invasive fungal infection of the paranasal sinuses, orbits, and brain. Rhino-orbital cerebral mucormycosis has increased in the recent second wave of post-COVID-19 illness (esp Delta strain) mainly in tropical countries like India [1]. The burden of diabetes mellitus and indiscriminate use of corticosteroid, environmental factors, post-COVID-19 immunological derangement might supposedly contribute to the development of extensive outbreak of ROCM [2]. Cerebrospinal Fluid (CSF) rhinorrhoea is the leakage of CSF from the subarachnoid space into the nasal cavity. Cerebrospinal fluid rhinorrhea is rarely documented with such fungal infection in literature. There are only a few case reports of iatrogenic CSF rhinorrhea in ROCM during orbital exenteration and paranasal sinus surgery [3].
Case description
A 40-year-old female patient with a five-year history of diabetes, a one-year history of hypertension, and a recent acute COVID-19 pneumonia reported with per-nose discharge for 20 days. The discharge was clear, colorless, and odorless, and it increased as the head was bowed forward. It was accompanied by severe swelling of the left face and a low-grade temperature. After 12 days, there was acutely progressing painful swelling of the left eye with foul-smelling ocular discharge. There were no symptoms of sensorium impairment, headache, seizures, vomiting, vision loss, or weakness. The general examination of the patient was normal. Local examination revealed tenderness in the left-sided paranasal sinuses, as well as induration across the left maxillary region. The oral examination was normal. A neurological examination revealed left-sided external ophthalmoplegia with chemosis and conjunctival injection (Figure 1a). The remainder of the nervous system, including other systems, was found to be normal.
On further evaaluation, there was presence of microcytic-hypochromic anemia, leukocytosis, random blood glucose of 461 mg/dL, C-Reactive protein 26.9 mg/L, HbA1C 11.3% with normal renal, liver, thyroid function and electrolyte levels. She was serologically negative for HBsAg, Anti-HCV, HIV. Her cerebrospinal fluid examination was normal. The nasal discharge was positive for beta-2 transferrin. Magnetic Resonance Imaging (MRI) of paranasal sinuses revealed left maxillary, sphenoid, frontal and bilateral ethmoidal sinusitis along (Figure 1b,1c,1d,1e) with focal erosion of left cribriform plate (Figure 1f). The left-sided pre-maxillary soft tissue along with masticatory spaces showed radiological involvement along with presence of right-sided mastoiditis. MRI of orbit showed erosion of left inferior orbital wall to involve extraconal fat with involvement of left-sided inferior rectus muscle. Her computerized tomography of paranasal sinuses showed mucosal thickening in the left maxillary, ethmoidal and frontal sinuses, obliteration of osteomeatal complexes, with a defect in left-sided cribriform plate (Figure 1g). MRI of brain was normal. Functional Endoscopic Sinus Surgery (FESS) showed left-sided greyish-brown crusts with congestion suggesting maxillary sinusitis (Figure 2a). Histopathological examination of nasal tissue was positive for broad-based aseptate fungal hyphae branching at acute-angle resembling mucormycosis, moderate lymphoplasmacytic inflammatory infiltrates and extensive necrosis (Figure 2b).
She was diagnosed as ROCM and treated with liposomal amphotericin-B therapy for six weeks with a single retrobulbar amphotericin-B injection, then oral posaconazole therapy for three months. An aggressive Functional Sinus Endoscopic Surgery Debridement (FESS) was performed to extensively remove the necrotic tissues and discharge from the paranasal sinuses. Euglycaemia was maintained with Insulin followed by oral antidiabetic medication.
CSF rhinorrhea resolved within seven days of intravenous amphotericin-B therapy. Her left-sided orbital swelling completely subsided over 14 days, while ocular movements returned to normal over a month (Figure 3). Sinusitis recovered over three months of antifungal treatment. On follow-up at 3 months, the patient was found to be completely normal clinically, along with total resolution of previous MRI lesions of paranasal sinuses, orbit and brain without evidence of any new lesion.
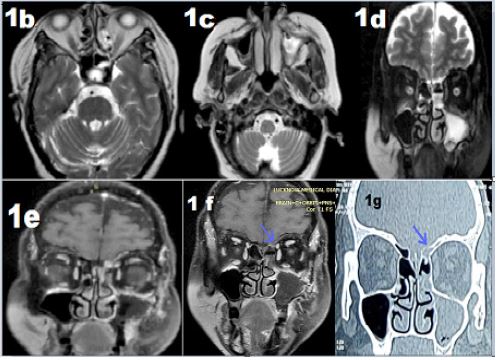
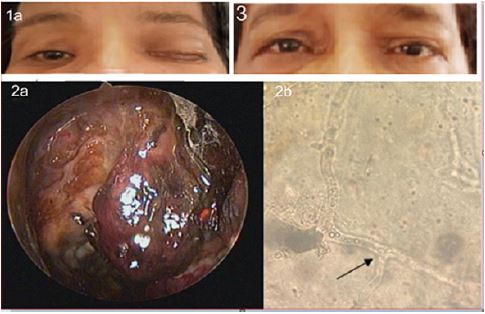
Figure 2: (a) Nasal endoscopic view showing necrotic tissue over middle turbinate and cribriform area,
(b) KOH mount showing broad aseptate right angle branching (Black arrow) fungal hyphae of Mucormycetes.
Figure 3: Showing resolution of ocular swelling, ptosis and chemosis.
Discussion
This case report describes the clinical course of a 45-year-old diabetic female with post-COVID-19 illness suffering from ROCM presenting with spontaneous CSF rhinorrhea. Spontaneous CSF rhinorrhea is a rarely reported phenomenon during an epidemic of ROCM.
The COVID-19 disease affects CD4+/CD8+ T-cells and antigen-presenting cells, favoring the development of secondary fungal infections [4]. The pathogenesis of delta strain of COVID-19 for the development of Coronavirus (COVID-19)-associated Mucormycosis (CAM) is multifactorial, namely, endothelial injury, enhancement of endothelial receptor expression of Angiotensin-Converting Enzyme 2 receptor (ACE2) and Glucose Regulated Protein Receptor (GRP78), immune dysregulation, oxidative stress, etc. This leads to increased epithelial interactions and endothelial invasion of mucorales spores which is the crucial step for angio-invasion and tissue necrosis in ROCM [5]. Mucormycosis is referred to as a diabetes-defining illness. Mucormycosis is an angio-invasive disease caused by saprophytic fungi of Mucorales order, ubiquitously present in nature. Diabetes mellitus is an important predisposing factor. Brain involvement occurs primarily by direct contiguous spread from paranasal sinuses (70%) and hematogenous route (30%) [2].
CSF Rhinorrhoea can be congenital or acquired by trauma (80-90%), neoplastic, or spontaneously (3-4%) [3]. The pathogenesis might be due to direct fungal osteodural invasion to cause trickling-out of CSF. In addition, many cases go unrecognized due to concurrent sinusitis during ROCM. These defects can lead to life-threatening severe ascending brain infections [4]. Early aggressive surgical debridement of infected tissues, early initiation of antifungals and euglycemia are the main pillars in management. Liposomal amphotericin-B constitutes first-line treatment followed by posaconazole and isavuconazole. Intraocular (retrobulbar) amphotericin-B injection has emerged as a promising nonsurgical therapy by halting orbital disease progression and preserving the globe [6]. Improving the survival rate requires rapid diagnosis and early therapeutic interventions with multidisciplinary team effort.
References
- Sen M, Honavar SG, Bansal R, et al. Epidemiology, clinical profile, management, and outcome of COVID-19-associated rhino-orbital-cerebral mucormycosis in 2826 patients in India- Collaborative OPAI-IJO Study on Mucormycosis in COVID-19 (COSMIC), Report 1. Indian J Ophthalmol. 2021; 69: 1670-1692.
- Bhattacharyya A, Sarma P, Kaur H, et al. COVID-19 associated rhino-orbital-cerebral mucormycosis: A systematic review, meta-analysis, and meta-regression analysis. Indian J Pharmacol. 2021; 53: 499-510.
- Arora K, Mehta A, Virk RS, et al. Cerebrospinal fluid leak from lateral orbit during exenteration for mucormycosis. BMJ Case Rep. 2020; 13: e237575.
- Chikley A, Ben-Ami R, Kontoyiannis DP. Mucormycosis of the central nervous system. J Fungi. 2019; 5: 59.
- Prakash H, Skiada A, Paul RA, Chakrabarti A, Rudramurthy SM. Connecting the dots: interplay of pathogenic mechanisms between COVID-19 disease and Mucormycosis. Journal of Fungi. 2021; 7: 616.
- Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019; e405-421.