
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Embolization of giant hepatic hemangioma: A case report
Gabriela Azevedo Solino1*; Izabel Graceli Pereira Santos 2; Mariana Poltronieri Pacheco3
11Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória, EMESCAM - Departamento de Medicina - Vitória, Espírito Santo - Brazil.
22Hospital Santa Casa de Misericórdia de Vitória - Departamento de Residência de Clínica Médica - Vitória, Espírito Santo - Brazil.
33Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória, EMESCAM – Departamento de Gastroenterologia e Hepatologia – Vitória, Espírito Santo – Brazil.
*Corresponding Author : Gabriela Azevedo Solino
Escola Superior de Ciências da Santa Casa de Misericórdia de Vitória, EMESCAM - Departamento de Medicina - Vitória, Espírito Santo - Brazil.
Email: gabrielaazesolino@gmail.com
Received : Feb 27, 2023
Accepted : Mar 14, 2023
Published : Mar 21, 2023
Archived : www.jcimcr.org
Copyright : © Solino GA (2023).
Abstract
Introduction: Hepatic hemangiomas (HH) are the most common benign tumors of the liver and consist of vascular malformations or hamartomas of congenital origin that increase due to ectasia. The declared giant hepatic hemangiomas (GHH) embody from 10 cm (most commonly) to 20 or more cm. In general, most patients are asymptomatic and the diagnosis is usually made accidentally by imaging tests.
Objective: To report a case of GHH embolization and share it with the medical and scientific community in order to expand knowledge about this pathology and benefit patients affected by this disease.
Case report: 63-year-old male with weight loss, lack of appetite, early satiety and postprandial fullness for 1 year associated with a painful and palpable abdominal mass. Computed tomography (CT) of the abdomen was performed, which showed a large expansive formation compatible with GHH. The patient underwent embolization by arteriography, with partial improvement of symptoms but without reduction in the size of the lesion.
Conclusion: The literature is scarce about the treatment and follow-up of patients with GHH, and it should be individualized on a case-by-case basis. Embolization is the minimally invasive and successful therapeutic choice. Hence, it is essential to contribute data regarding this pathology to the scientific community, as guidance to determine the preferred conduct in HHG cases.
Keywords: Cavernous hemangioma; Giant hepatic hemangioma; Arterial embolization; Surgery.
Abreviations: CHC: Carcinoma Hepatocellular; cm: Centimeters; CT: Computed Tomography; GHH: Giant Hepatic Hemangiomas; HH: Hepatic Hemangiomas; mm: Millimeters; MRI: Magnetic Resonance Imaging; TAE: Transarterial Embolization.
Citation: Solino GA, Santos IGP, Pacheco MP. Embolization of giant hepatic hemangioma: A case report. J Clin Images Med Case Rep. 2023; 4(3): 2334.
Introduction
Hepatic Hemangiomas (HH) are the most common benign tumors of the liver, representing approximately 0.4-20% according to data in the literature, while necropsy data show a frequency of 0.4-7.3% [1-3]. They consist of clusters of vessels, lined by a single layer of endothelial cells within a thin fibrous stroma and fed by the hepatic artery [1,4]. Regarding classification by size, there is no very well-defined consensus in the literature, but the most accepted today are that the small HH, can range from a few millimeters (mm) to 3 centimeters (cm); the medium ones ranging from 3-10 cm and the so-called giant hepatic hemangiomas (GHH) with 10 cm (most commonly) up to 20 cm or more [1,5].
In general, most patients are asymptomatic, however, multiple or giant HH may have symptoms such as abdominal pain, nausea, vomiting, lack of appetite and post prandial fullness [1,4,6]. The diagnosis is usually made accidentally by imaging tests [1,4], and suspected in cases where there is solid liver damage in non-cirrhotic patients and in the absence of extrahepatic malignancy [7].
The present study aimed to report a case of GHH in a patient treated at Hospital Santa Casa de Misericórdia de Vitória, in Espírito Santo, Brazil.
The study was submitted to the Ethics Committee, with approval from the Institution (CAAE: 64725022.5.0000.5065, approval 5.747.317).
Case report
63-year-old male, bus driver, with no known comorbidities, with unintentional weight loss of 12 kg, lack of appetite, early satiety and postprandial fullness for 1 year. On physical examination, there was a palpable and painful abdominal mass occupying the epigastric region, and hypochondrium and right flank. Full abdomen Computed Tomography (CT) was requested, which showed a large heterogeneous expansive formation occupying the entire right hepatic lobe, determining partial compression of segment IV, with defined contours, measuring about 23 x 23 x 23 cm, exhibiting peripheral, globuliform, and centripetal contrast enhancement, with some liquefied/necrotic areas in between, suggestive of GHH (Figure 1).
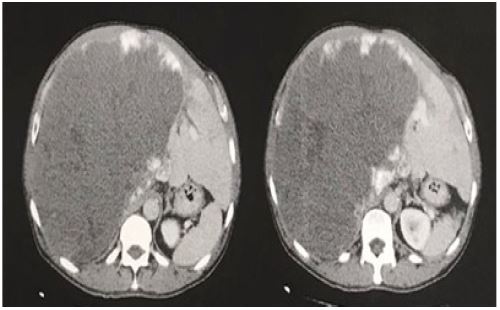


After diagnosis, Transarterial Embolization (TAE) of the lesion was performed, with catheterization of the right hepatic artery showing multiple nodular images, procedure performed without complications. The patient returned to the service 1 month after the procedure, referring partial improvement of the previously reported symptoms and with control images that did not show a reduction in lesion size, comprising almost the entire right hepatic lobe with the same aspects described previously, and the current image showed small enlargement of the area with central cystic/necrotic degeneration (Figures 2 and 3).
During follow up, a new abdominal CT scan and doctors appointment were performed 7 months after TAE, still referring inappetence, abdominal pain with efforts and postprandial fullness. On the imaging examination, it presented voluminous hemangioma with calcium foci of permeation occupying the entire right lobe, and the medial segments of the left lobe measuring 24.5 x 22.5 x 21 cm, showing that there was no reduction in GHH after the procedure.
Discussion
HH, despite having an uncertain etiology, are considered as vascular malformations or hamartomas of congenital origin that increase due to ectasia [7]. Its highest incidence occurs in the elderly and women, in a ratio of 6 women: 1 men [5,6] and, it is believed that they can increase in size during pregnancy or with the use of estrogen therapy. The GHH are those that have from 10 (most commonly) to 20 or more cm in size and are present in less than 10% of cases [1,5].
Usually symptoms and complications depend on the size and location. In most cases, they are asymptomatic, and, when symptomatic, especially in GHH or multiples, may course with abdominal pain or discomfort, nausea, vomiting, lack of appetite and postprandial fullness [1,4,6]. Rarely, acute abdominal pain may occur, usually associated with injury thrombosis or bleeding, leading to distention of the hepatic capsule [7].
The physical examination, for the most part, also appears unchanged, except in cases of GHH in which there may be liver or a palpable mass, as well as the normality of laboratory tests, unless there are complications such as thrombosis, hemorrhages and compression of the bile duct structures [1,4]. Similar to the reported case, the patient had the nonspecific symptomatology of a GHH, in addition to a painful palpable mass in the abdomen.
Complications are rare and can be divided into: acute or chronic inflammatory (fever), mechanical (spontaneous or traumatic rupture, compression of adjacent structures) and bleeding, may have concomitant coagulopathies such as Kassabach Merritt syndrome, characterized by the association of HH, thrombocytopenia and intravascular coagulation [1].
The diagnosis, usually accidental, can be performed with ultrasonography if there are classic characteristics such as homogeneous margin, hyperechoic and well-delimited and smaller than 3 cm. If these criteria do not exist, contrast tests are necessary, such as CT or Magnetic Resonance Imaging (MRI), which a sensitivity of approximately 90% and a specificity of more than 90%, wich can also make the differential diagnosis with other liver lesions such as hepatocellular carcinoma (HCC) [7].
The classic image in a hh in CT is characterized as a hypodense, well-defined lesion, with peripheral nodular enhancement with centripetal homogeneous filling, as well as the image evidenced in the reported case. Liver biopsy is usually not used as there is a risk of rupture with bleeding, which may lead to hemodynamic instability, in addition to having a low diagnostic performance [7].
Treatment depends on the existence of symptoms. If asymptomatic, hh does not require treatment and surveillance with imaging tests will be carried out, depending on the size of the lesion, usually when greater than 5 cm [7]. If there are symptoms, such as pain refractory to analgesia, and these are persistent and attributed to HH, or rapid growth, intratumoral risk of thrombosis or rupture, the approach should be considered. Therapeutic methods can be surgical or radio-interventional.
Regarding surgery, we have liver resection, enucleation and liver transplantation as an option [5,8]. The choice between the current methods is not completely defined in the literature and it depends on the location, size, number of HH, patient conditions and the preference and experience of the doctor.
In many centers, the surgical option is the first choice of treatment for HH with lesions of limited size, however, in cases of GHH and/or multiples, there is still no consensus in the world literature, which leads to a dilemma in clinical practice, as its management is individualized on a case-by-case basis. In cases where the surgical option is indicated, it is known that there is a high risk of complications such as excessive bleeding, prolonged hospital stay, significant loss of liver parenchyma with the possibility of progression to liver failure and a mortality rate of 0.5-2% that should be considered [8].
Some studies show that most surgeons prefer enucleation over resection, due to the ease and speed of the method, in addition to less blood loss. In a study used as a reference, in which 144 elective GHH surgeries were performed, there was no significant difference in relation to the two techniques, when comparing the surgical time, amount of blood loss and transfusion need, in addition to postoperative complications and hospitalization time [9].
The indication for liver transplantation in cases of HH occurs mainly in cases related to rapid and significant growth of the mass at risk of rupture, severe coagulopathies, severe and persistent abdominal pain, respiratory distress or failure of previous interventions. According to the consulted literature, there are approximately 19 cases of liver transplantation by GHH, being the main indication Kassabach Merritt syndrome, contemplating a total of 10 cases [10].
Due to recent technological advances, radio-interventional techniques were developed as an alternative approach to surgical methods, which are currently used in those multiple and/or giant lesions and include TAE, ablation, percutaneous sclerotherapy and percutaneous argon-helium cryotherapy [5,8]. These have the advantages of being less painful, minimally invasive and very efficient [6]. However, they are also at risk of complications, such as post-embolization syndrome, biloma, liver abscess, hydrothorax, and ischemia with portal necrosis [8].
Although technological advances have made radio intervention possible as an excellent therapeutic possibility for HH, TAE in many of the reports in the literature was used as a bridge to tumor reduction in those considered unresectable allowing subsequent resection with greater ease and safety [2,11].
In the case reported here, we chose to perform the TAE because it was a GHH measuring 23 x 23 x 23 cm, evaluating the risks and benefits of the other modalities and the indications of each therapeutic option.
In the literature, there is still no consensus on the ideal follow-up time with patient control tests, however, in the works found, most of them carry out the follow-up 6 months after the procedure [12,13]. Early images may be the reason for not observing tumor reduction, and, if kept unchanged during the following months of follow up, new therapeutic approaches must be considered.
Conclusion
GHH is a rare pathology and, as a result, the literature is scarce, both regarding treatment modalities and patient follow-up mode, each case should be individualized and the risks and benefits of therapeutic options assessed, in addition to existing knowledge on the subject.
Both surgery and arterial embolization are treatment options for GHH. However, considering the high risk of complications from surgical intervention, embolization is currently presented as a minimally invasive choice with successful therapeutic targets.
Therefore, it is essential to contribute data about this pathology to the scientific community, assisting in defining the preferred conduct in GHH cases.
Funding : Not applicable.
Acknowledgements : Not applicable.
References
- Bajenaru N, Balaban V, Săvulescu F, Campeanu I, Patrascu T. Hepatic hemangioma -review-. J Med Life. 2015; 8: 4-11.
- Sun J-H, Nie C-H, Zhang Y-L, Zhou G-H, Ai J, et al. Transcatheter Arterial Embolization Alone for Giant Hepatic Hemangioma. PLoS ONE. 2015; 10: e0135158.
- Ketchum WA, Lin-Hurtubise KM, Ochmanek E, Ishihara K, Rice RD. Management of Symptomatic Hepatic “Mega” Hemangioma. Hawaii J Med Public Health. 2019; 78: 128-131.
- Sociedade Brasileira de Hepatologia. Diagnóstico e tratamento de nódulos hepáticos benignos Recomendações da Sociedade Brasileira de Hepatologia - SBH. 2014.
- Xie QS, Chen ZX, Zhao YJ, Gu H, Geng XP, Liu FB. Outcomes of surgery for giant hepatic hemangioma. BMC Surg. 2021; 21: 186.
- Jia K, Gao Z, Li M, Yu C. Interventional treatments for hepatic hemangioma: A state-of-the-art review. J Interv Med. 2022; 5: 6-9.
- Curry MP, Chopra S. Hepatic Hemangioma. Up to Date. 2021.
- Dong W, Qiu B, Xu H, He L. Invasive management of symptomatic hepatic hemangioma. Eur J Gastroenterol Hepatol. 2019; 31: 1079-1084.
- Abdel Wahab M, El Nakeeb A, Ali MA, Mahdy Y, Shehta A, Abdulrazek M, et al. Surgical Management of Giant Hepatic Hemangioma: Single Center’s Experience with 144 Patients. J Gastrointest Surg. 2018; 22: 849-858.
- Zhao Y, Li XP, Hu YY, Jiang JC, Zhao LJ. Liver transplantation for giant hemangioma of the liver: A case report and review of the literature. Front Med (Lausanne). 2022; 9: 985181.
- Akamatsu, N., Sugawara, Y., Komagome, M. et al. Giant liver hemangioma resected by trisectorectomy after efficient volume reduction by transcatheter arterial embolization: a case report. J Med Case Reports. 2010; 4: 283.
- Ozgur O, Sindel HT. Giant hepatic hemangioma treatment with transcatheter arterial embolisation and transcatheter arterial chemoembolisation; Comparative results. Turk J Med Sci. 2021; 51: 2943-2950.
- Oldhafer KJ, Habbel V, Horling K, Makridis G, Wagner KC. Benign Liver Tumors. Visc Med. 2020; 36: 292-303.