
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Inflammatory fibroid polyp presenting as intussusception
Nidhi Aley Alex1*; Sankar S2
1Junior Resident, Department of Pathology, Government Medical college, Kottayam, Kerala, India.
2Professor, Department of Pathology, Government Medical College, Kottayam, Kerala, India.
*Corresponding Author : Nidhi Aley Alex
Junior Resident, Department of Pathology, Government Medical college, Kottayam, Kerala, India.
Email: alexnidhi@yahoo.com
Received : Mar 02, 2023
Accepted : Mar 21, 2023
Published : Mar 28, 2023
Archived : www.jcimcr.org
Copyright : © Alex NA (2023).
Abstract
Inflammatory fibroid polyp is a benign mesenchymal tumor most commonly arising in the stomach and ileum. It needs to be distinguished from other mesenchymal tumors of the GIT which is done with the help of morphological features and with the help of IHC. Here in, we describe the case of a 58 year old female who presented with complaints of abdominal pain, contrast- enhanced computed tomography revealed a target- like structure which was consistent with intussusception due to the lesion. Following surgery and histopathological examination of the specimen and IHC study, diagnosis of IFP was made.
Keywords: fibroid polyp; Onion skin fibrosis; CD34, SMA.
Citation: Alex NA, Sankar S. Inflammatory fibroid polyp presenting as intussusception. J Clin Images Med Case Rep. 2023; 4(3): 2344.
Introduction
Inflammatory fibroid polyp is a benign polypoidal fibroblastic neoplasm. It is most commonly seen in the stomach followed by ileum, however they may arise anywhere in the gastro intestinal tract. Patient presents with abdominal obstruction, pain or bleeding and if the tumor arises from small intestine intussusception is a common presentation. It arises from submucosa and often the mucosal surface will show ulceration. In tissue sections, proliferation of spindle myofibroblast cells are seen with stroma containing inflammatory infiltrate predominantly eosinophils and lymphocytes. Small and medium sized blood vessels typically show concentric fibrosis (onion skin fibrosis).
The pathogenesis is unclear. Studies recently have reported a possible sharing of the PDGFRA mutational profile with Gastro Intestinal Stromal Tumour (GIST) particularly exons 12 and 18 [1,2]. By Immunohistochemistry, there is consistent positivity for CD34, and variable immunoreactivity with SMA. KIT, DOG1, Desmin, S100 and keratins are negative.
Case report
A 58 year old female patient who is a known case of systemic hypertension presented to casualty with complaints of abdominal pain and nausea for the past 4 months, aggravated since 2 weeks. On examination, abdomen was distended, however there was no tenderness. Her vitals were normal and there was no history of gastrointestinal bleeding or vomiting.
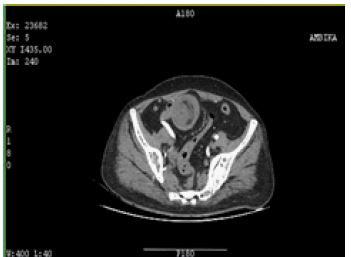
Image findings showed a well-defined homogenous soft tissue density lesion in the mid jejunal loop measuring 3.8 x 3.9 x 3.4 cm which appears to be lead point of jejunojejunal intussusception measuring a length of 14 cm.
She underwent small bowel resection, the intraoperative findings of which were small bowel tumor with stricture 50 cm from jejunum, with stricture in the proximal part and serosal involvement distally. Small bowel resection and end to end jejunostomy was performed. The specimen was sent for histopathological examination.
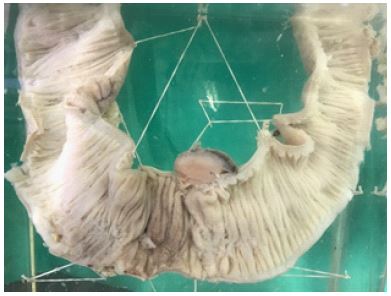
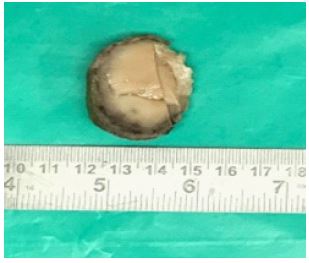
Grossly we received a segment of small intestine with an iatrogenic rent through which a polypoidal mass with a stalk was protruding measuring 4.1 x 3.5 x 3 cm which is at a distance of 24.5 cm from proximal end, cut section of this polypoidal mass was fleshy appearance.
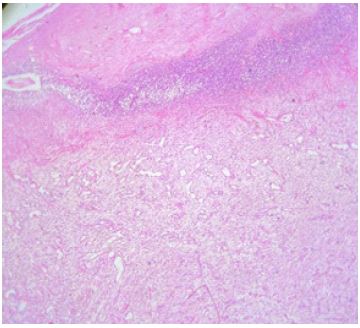
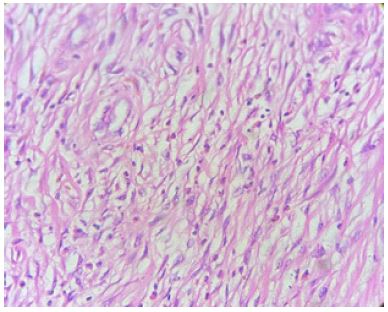
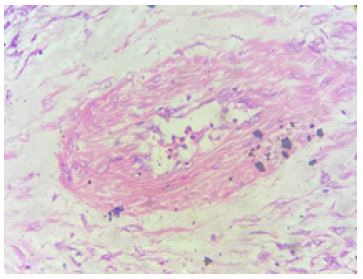
Microscopical examination showed a polypoidal lesion arising from submucosa with individual cells ovoid/spindle with scanty to moderate cytoplasm, bland vesicular nucleus and indistinct nucleoli. Stromal cells are admixed with inflammatory cells predominatly eosinophils and proliferated blood vessels. Focal onion skin fibrosis around blood vessels noted. Tip of the polyp is necrosed (gangrenous). Both resected ends are viable. The attached mesentry shows 13/13 lymph nodes with reactive change only.
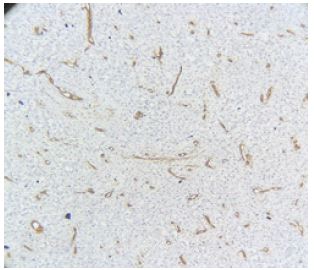
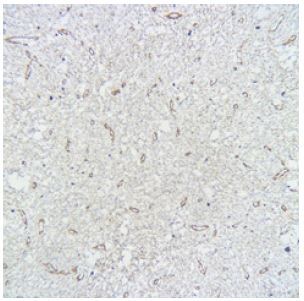
Immunohistochemistry was done. Spindle cells are positive for SMA, negative for CD117, CD34, Ki67- 10% consistent with Inflammatory fibroid polyp.
Discussion
The presentation of inflammatory fibroid polyp depends on the location of the tumor. Studies show that in patients with lesions involving the stomach they present with abdominal pain and in patients with small intestinal lesions, they present with obstruction as a sequel of intussusception as in our case report. For decades inflammatory fibroid polyps have been considered a reactive change of the gastric mucosa but recently the discovery of PDGFRA mutations has considered it to be a neoplastic process [3].
They are considered as a benign and non invasive lesion. However there has been a case report of transmural proliferation of the IFP with destruction of the muscularis propria extending to the serosa in literature which is a rare observation [4]. In study conducted Liu TC et al, Onion skin fibrosis around vessels which is a unique feature was observed in 54% (45 out of 83) of cases studied and is thus not always a reliable diagnostic feature [5].
IHC is essential to diagnose IFP because they tend resemble morphologically other mesenchymal tumors such as GIST, desmoid fibromatosis, Inflammatory Myofibroblastic tumour (IMT), leiomyoma, and schwannoma among others which are the histopathological differentials of IFPs [6]. Most IFPs are positive for CD34, whereas about 10%-20% of cases show focal reactivity for SMA and desmin. C-KIT (CD117), DOG1, and S-100 are consistently negative [7]. Hasegawa et al studied 11 cases of inflammatory fibroid polyps of the stomach, in which they concluded that CD34 expression is a reliable IHC marker as it was observed in 100% of the cases studied [8]. In our case, however onion skinning was observed and the presence of many eosinophils combined with SMA positivity lead to the diagnosis of IFP.
References
- Bjerkehagen B, Aaberg K, Steigen SE. Do not be fooled by fancy mutations: Inflammatory fibroid polyps can harbor mutations similar to those found in GIST. Case reports in medicine. 2013; 2013: e845801.
- Lasota J, Wang ZF, Sobin LH, Miettinen M. Gain-of-function PDGFRA mutations, earlier reported in gastrointestinal stromal tumors, are common in small intestinal inflammatory fibroid polyps. A study of 60 cases. Mod Pathol. 2009; 22: 1049–1056.
- Nonose R, Valenciano JS, Silva CMG da, Souza CAF de, Martinez CAR, et al. Ileal Intussusception Caused by Vanek’s Tumor: A Case Report. CRG. 2011; 5: 110–116.
- Tajima S, Koda K. Locally infiltrative inflammatory fibroid polyp of the ileum: Report of a case showing transmural proliferation. Gastroenterology Report. 2018; 6: 144–148.
- Liu TC, Lin MT, Montgomery EA, Singhi AD. Inflammatory Fibroid Polyps of the Gastrointestinal Tract: Spectrum of Clinical, Morphologic, and Immunohistochemistry Features. The American Journal of Surgical Pathology. 2013; 37: 586–592.
- Karuhanga T, Ngimba C, Yahaya JJ. Inflammatory Fibroid Polyp in 48-Year-Old Male: A Rare Cause of Intussusception. Case Reports in Surgery. 2020; 2020: e9251042.
- BP Rubin and JL Hornick. Mesenchymal tumors of the gastrointestinal tract, in practical soft tissue pathology: A diagnostic approach, Elsevier. 2019; 214: 459–498.
- Hasegawa T, Yang P, Kagawa N, Hirose T, Sano T, et al. CD34 expression by inflammatory fibroid polyps of the stomach. Mod Pathol. 1997; 10: 451–456.