
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Commentary - Open Access, Volume 4
Let’s know systemic lupus erythematosus
Jayesh Trivedi1*; Twinkle Rana2; Shailj Ani2; Parth Rathva3; Mayur Patel3
1Head of Department and Professor, General Medicine, Gujarat Adani Institute of Medical Sciences, India.
2Third Year Resident, General Medicine, Gujarat Adani Institute of Medical Sciences, India.
3Second Year Resident, General Medicine, Gujarat Adani Institute of Medical Sciences, India.
*Corresponding Author : Jayesh Trivedi
Head of Department and Professor, General Medicine, Gujarat Adani Institute of Medical Sciences.
Email: drjvtrivedi@rediffmail.com
Received : Mar 08, 2023
Accepted : Mar 22, 2023
Published : Mar 29, 2023
Archived : www.jcimcr.org
Copyright : © Trivedi J (2023).
Citation: Trivedi J, Rana T, Ani S, Rathva P, Patel M. Let’s know systemic lupus erythematosus. J Clin Images Med Case Rep. 2023; 4(3): 2345.
Introduction
Systemic Lupus Erythematosus (SLE) is an autoimmune disease with a wide spectrum of disease expression, with aberrant host innate and adaptive immune response, and chronic inflammation. It is a chronic autoimmune inflammatory disease with a spectrum of clinical and serological manifestations caused by autoantibody production, complement activation, and immune complex deposition. The etiopathogenesis of SLE is entirely not clear, but is believed that it results from the complex interaction between genetic and hormonal factors, and environmental exposures. SLE has an unpredictable course that represents a challenge in the understanding of this disease. Efforts are directed toward the identification of its different pathogenic pathways, which allows evaluating the activity and progression of the disease and its responses to the different therapeutic approaches.
Pathogenesis
The pathogenesis of SLE is characterized by the formation of autoantibodies and a breakdown in the immune milieu of the body leading to an unregulated inflammatory response. This is a result of the interplay between genetic susceptibility, environmental factors, and hormonal influence. The genes involved play a role in immune autoregulation. The autoantibodies and the resultant inflammatory state is how the disease process is initiated and maintained throughout its natural history.
Infections like the Epstein–Barr Virus (EBV) and Cytomegalovirus (CMV) have been associated with SLE. EBV, where molecular mimicry (EBNA-1, an EBV protein, can cross-react with an autoantigen, Ro] is known to trigger a flare.
10-fold increased risk of SLE among monozygotic twins compared to dizygotic twins, in addition to an obvious aggregation of SLE in families. This evidence together with variability among ethnic populations strongly supported a genetic component in the pathogenesis of SLE. The complex pathogenesis of SLE seems to be the cumulative effect of multiple proteins that have a role in innate and adaptive immunity (including immune complex processing, clearance of cellular debris, type I Interferon (IFN) and Toll-Like Receptors (TLR) signalling, and lymphocyte activation).
Exposure to silica dust and smoking have been defined as established risk factors for SLE. With regards the role of silica exposure in SLE, its deregulatory role in the immune system causes increased proinflammatory cytokines, oxidative stress, and induction of apoptosis and release of intracellular antigens. Drugs are a major factor, and the common drugs implicated are hydralazine, D-penicillamine, minocycline, lithium, and more recently, Tumor Necrosis Factor alpha (TNF-ɑ) blocking agents.
Classification criteria
The Systemic Lupus International Collaborating Clinics (SLICC) group introduced a set of validated criteria with higher sensitivity than the revised American College of Rheumatology criteria. The American College of Rheumatology included fluorescence antinuclear antibody and antibody to native DNA and Sm antigen. Some criteria were redefined (neurological involvement, arthritis) while others were reorganized to reduce redundancy (photosensitivity, malar rash). Antinuclear Antibodies (ANA), anti-double-stranded DNA antibodies (anti-ds DNA) and Anti Phospholipid Antibodies (APLA) are among the antibodies that are now considered for different inclusion criteria, each one of which may contribute to the classification. Low complement level has also been recently added.
To label a patient as having SLE, at least four criteria from the combined list of clinical and immunological criteria should be present, including one clinical and one immunological criterion, according to the SLICC criteria. If the patient has biopsy-proven Lupus Nephritis (LN) with a positive ANA and anti-ds DNA, then that is sufficient to call it SLE. The requirement of one clinical and one immunological criterion is to avoid patients without clinical features or antibodies.
Pathology and management
SLE is characterized by periods of remission and exacerbation with prolonged periods of subclinical activity, thus making it a very unpredictable disease. It can affect almost every organ in the body, more so during a flare. In milder versions of the disease, joints and skin are the main affected organs. In moderate forms, more organs are involved, but it is the severe form where the heart and kidneys are affected that makes this disease so lethal. Approximately 35%-52% of these patients have renal involvement, and it is usually reported in the early phase of the disease, so measures must be taken to prevent organ damage since this condition is clinically silent. Anti-Smith antibodies, anti-C1q antibodies, low complement, and anti-dsDNA are associated with renal involvement.
Neuropsychiatric SLE may present in many forms, it can involve the central and peripheral nervous systems with either a focal or diffuse syndrome. Headaches, although they are a frequent manifestation, have no relation to the activity of the disease; however, the clinician must remain alert to the possibility of subarachnoid hemorrhage or cortical venous thrombosis. “Brain fog,” cognitive decline, and depression are also common.
Gastro Intestinal (GI) symptoms and hepatic features are present in 40%–70% of patients. These together with the cardiovascular manifestations must be distinguished from those produced by infections, comorbid conditions, and adverse drug events.
The use of immunosuppressant drugs, the presence of certain SLE-related autoantibodies, chronic immune dysregulation, environmental factors, and shared genetic susceptibility are among the factors that potentially mediate malignancy risk in patients with SLE.
Investigations
Lab investigation-CBC may show lymphopenia, thrombocytopenia, anemia. Liver enzymes can be elevated, CRP will be normal and ESR will be elevated. Patient may have Hemolyticanemia which is coombs test negative. ANA profile will have anti DsDNA Positivity and anti SM which is more specific.
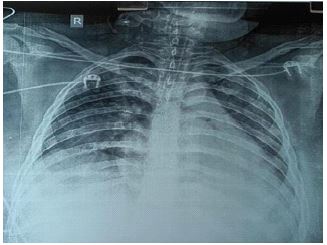
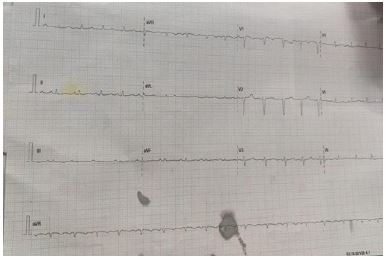
Clinically there will be involvement of Pericardium, Peritoneum and the pleural resulting in polyserositis. We also came across one of our SLE patient who was having Biventricular failur, pulmonaryedema, hypoproteinemia, pericardial effusion and her eGFR was 45. On further Investigation, on chest XRAY had cardiomegaly with right sided pleural effusion. On Ecg there was low voltage complexes.
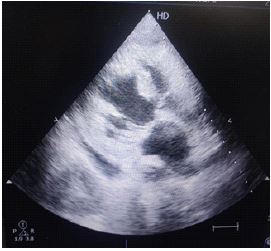
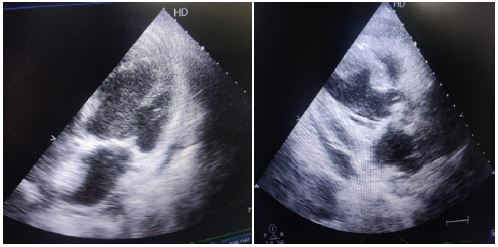
On 3d echo examination we noticed concentric hypertrophy of IVS LVPW with vegetation on anterior mitral leaflet on the atrial surface with mild pericardial Effusion, this vegetation was almost 5 mm, aortic valve revealed trivial aortic regurgitation with thickening of endocardium such endocarditis is known as non infective endocarditis-Libman Sack’s Endocarditis.
This is a known entity in medical science, here the blood culture for anaerobic, aerobic and fungal were negative. On USG chest and abdomen-right sided pleural effusion, ascites and cortical thickening of the renal parenchyma and altered corticomedullary ratio was seen. Urine routine micro showed aseptic pyuria.
Treatment
The treatment for this malady depends on the organs and systems involved as well as the severity. It can include topical applications for skin problems, nonsteroidal anti-inflammatory drugs for musculoskeletal diseases, and immunosuppression.
Hydroxychloroquine has been noticed to have immunomodulatory properties that are used to treat arthritis and cutaneous flares, protect against ultraviolet rays, improve sicca symptoms, treat milder disease, and improve the cardiovascular profile of a patient by reducing cholesterol, the risk of diabetes, and carotid plaque development; it also has antithrombotic properties. Furthermore, it can also be indicated during pregnancy or lactation. There is also a rare risk of retinal toxicity.
Corticosteroids have an immunosuppressive and anti-inflammatory effect through the modification of genomic and non-genomic pathways. The organ system affected and the severity of the disease guide the dosage and administration route of the drug. In life-threatening or organ-threatening disease, intravenous methylprednisolone as pulsed therapy is used, while in mild disease, an antimalarial in conjunction with prednisolone 5–15 mg/day or a steroid-sparing agent is used. Poor responders to steroids and patients with particular manifestations of SLE benefit with a combination of steroids and other immunosuppressive drugs.
Immunosuppressive agents are frequently indicated to reduce the risk of long-term damage accrual, control active disease, and as steroid-sparing agents. Azathioprine is the most commonly used cytotoxic agent in lupus, and it is usually initiated for the control moderate activity of lupus, the prevention of flares, maintenance therapy after remission, and steroid dose reduction. Also, it is the preferred drug for fertility preservation and during pregnancy.
Cyclophosphamide is primarily used in the treatment of GI, muscle, and pulmonary manifestations. While mycophenolate mofetil was shown to be a good induction agent, when combined with steroids, it can reduce moderate and severe lupus disease activity, reduce renal and non-renal flares; it also aids in steroid dose reduction and is well tolerated. It is more effective than azathioprine and less toxic than cyclophosphamide. Cyclophosphamide and MMF are both contraindicated during pregnancy and lactation.
In refractory cases, other drugs can be used. Cyclosporin and tacrolimus inhibit calcineurin which in turn inhibits the production of cytokines and lymphocyte proliferation—especially T-helper cells. Cyclosporin is useful as a steroid-sparing agent in patients with normal renal function. There is some evidence to suggest that tacrolimus can be used in case of induction of LN.
References
- Hahn BH, McMahon MA, Wilkinson A, et al. American College of Rheumatology Guidelines for screening, case definition, treatment and management of lupus nephritis. Arthritis Care Res. 2012; 64: 797–808.
- Renaudineau Y, Pers JO, Bendaoud B, Jamin C, Youinou P, et al. Dysfunctional B cells in systemic lupus erythematosus. Autoimmun Rev. 2004; 3: 516–523.
- Cooper MA, Fehniger TA, Turner SC, et al. Human natural killer cells: A unique innate immunoregulatory role for the CD56 (bright) subset. Blood. 2001; 97: 3146–3151.
- Weening JJ, D’Agati VD, Schwartz MM, et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. J Am Soc Nephrol. 2004; 65: 521–530.
- Tench CM, McCurdie I, White PD, D’Cruz DP, et al. The prevalence and associations of fatigue in systemic lupus erythematosus. Rheumatology. Oxford; 2000: 1249–1254.
- Bernatsky S, Boivin JF, Joseph L, et al. An international cohort study of cancer in systemic lupus erythematosus. Arthritis Rheum. 2005; 52: 1481–1490.
- Rose T, Dörner T. Drivers of the immunopathogenesis in systemic lupus erythematosus. Best Pract Res Clin Rheumatol. 2017; 31: 321–333.
- Crow MK. Collaboration, genetic associations, and lupus erythematosus. N Engl J Med. 2008; 358: 956–961.
- Petri M. Clinical features of systemic lupus erythematosus. https://www.ncbi.nlm.nih.gov/pubmed/8519612. CurrOpinRheumatol. 1995; 7: 395–401.
- Ytterberg SR, Schnitzer TJ. Serum interferon levels in patients with systemic lupus erythematosus. Arthritis Rheum. 1982; 25: 401–406.
- Squatrito D, Emmi G, Silvestri E, Ciucciarelli L, D’Elios MM, et al. Pathogenesis and potential therapeutic targets in systemic lupus erythematosus: From bench to bedside. Auto Immun Highlights.