
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Rare association of a patient with multiple ischemic strokes
with thrombotic thrombocytopenic purpura and systemic
lupus erythematosus: A case report
Enrique Lorenzo C Panganiban, MD1*; Patrick M Yalung, MD1; Lina C Laxamana, MD1; Jay T Datukan, MD2; Juan Javier Lichauco, MD3; Mylene U Cornel, MD4
1Institute for Neurosciences, St. Luke’s Medical Center, and Global City, Philippines.
2Hematology-Oncology, St. Luke’s Medical Center, Global City, Philippines.
3Rheumatology, St. Luke’s Medical Center, Global City, Philippines.
4Cardiology, St. Luke’s Medical Center, Global City, Philippines.
*Corresponding Author : Panganiban C
Institute for Neurosciences, St. Luke’s Medical Center, Global City, Philippines.
Tel: +63 917 867 0878;
Email: elncpanganiban@stlukes.com.ph
Received : Mar 03, 2023
Accepted : Mar 22, 2023
Published : Mar 29, 2023
Archived : www.jcimcr.org
Copyright : © Panganiban ELC (2023).
Abstract
The Trial of ORG 10172 in Acute Stroke Treatment categorizes stroke etiology into large-artery atherosclerosis, small vessel occlusion, cardio-embolism, stroke of undetermined etiology, and stroke of other determined etiology with patients with hematological, and hypercoagulable states falling under the last category. Cases of Thrombotic Thrombocytopenic Purpura with stroke manifestations have been described mostly as large vessel occlusion. More uncommonly, TTP overlapping with Systemic Lupus Erythematosus presenting as multiple ischemic strokes, have not yet been widely published. In TTP, the deficiency of ADAMTS-13 enzyme in hibition causes the generation of large multimeric complexes yielding increased platelet adhesion, thrombi formation, blood vessel occlusion, and hence, stroke. The objectives of the reportare to share a case of a 50-year old female with TTP-SLE overlap revealing multiple small vessel ischemic infarcts on cranial imaging, exemplifying its rarity, and to provide insight that treatment with Therapeutic Plasma Exchange facilitates early return to the pre-morbid state. Work-up yielded TTP-SLE overlap as the stroke cause, when her ancillary tests showed positive Direct Coombs’ test, anemia, thrombocytopenia, hyperbilirubinemia, analysed erythrocytes on peripheral blood smear. Admitted for eight days, the patient was transfused with blood products and underwent TPE before being discharged with an Aspirin, Hydroxychloroquine, and tapering steroids for two weeks. This case highlights the uniqueness of TTP-SLE overlap leading to multiple ischemic strokes, and how TPE can addressstroke symptoms thus preventing further deterioration and morbidity.
Keywords: Stroke; Thrombotic thrombocytopenic purpura; Systemic lupus erythematosus.
Abbreviations: DAMTS-13–A: Disintegrin-Like Metalloprotease Domain With Thrombospondin Type 1 Motifs; ANA: Anti-Nuclear Antibody; LDH: Lactate Dehydrogenase; LVO: Large Vessel Occlusion; MAP: Mean Arterial Pressure; MPPT: Methylprednisolone Pulse Therapy; MRI/MRA: Magnetic Resonance Imaging/ Magnetic Resonance Angiography; NCCU: Neurocritical Care Unit; NIHSS: National Institutes Of Health Stroke Scale; PLASMIC Score: Platelet Count, Combined Hemolysis Variable, Absence Of Active Cancer, Stem-Cell Or Organ Transplant, MCV, INR, Creatinine; RNP: Ribonucleoprotein; SLE: Systemic Lupus Erythematosus; SLEDAI: SLE Disease Activity Index; TOAST: Trial Of ORG 10172 In Acute Stroke Treatment; TPE: Therapeutic Plasma Exchange; TTP: Thrombotic Thrombocytopenic Purpur.
Citation: Panganiban ELC, Yalung PM, Laxamana LC, Datukan JT, Lichauco Jj. Rare association of a patient with multiple ischemic strokes with thrombotic thrombocytopenic purpura and systemic lupus erythematosus: A case report. J Clin Images Med Case Rep. 2023; 4(3): 2346.
Introduction/background
The causes of stroke have been well-established by trials worldwide. The TOAST criteria classifies the etiologies of stroke into five major categories: Large-artery atherosclerosis, small vessel occlusion, cardio-embolism, stroke of undetermined etiology, and stroke of other determined etiology with a small percentage of patients with hematological disorders and hypercoagulable states falling under the last group [1]. Cases of TTP in association with SLE have rarely been described, and there is a tendency for the symptomatology to overlap [8]. More so, the rarity of this overlap occurs if TTP is the first mani festation of SLE [6]. Although not all need to be fulfilled for the diagnosis of TTP, the classic pentad of thrombocytopenia, microangiopathic hemolytic anemia, fever, acute kidney injury, and neurological symptoms, are a result an inherited deficiency or acquired inhibition of the enzyme ADAMTS-13 [8,10]. The authors identified the 29-exon gene encoding the protein to be the specific cause in generating large multimeric complexes leading to increased platelet adhesion, thrombi formation, hence, blood vessel occlusion. SLE, on the other hand, can cause systemic inflammation, endothelial activation, or prothrombotic states, and derangements in Virchow’s triad, creating a cellular environment that primes platelet activation, resulting to ischemia of the distal cerebral arteries [2,5]. To date, there have not been many published articles on large populations of patients with TTP and SLE leading to a stroke, and only closely related studies on TTP and stroke, or SLE and stroke have been documented.Articles showing case reports of LVOs in association with TTP were conveniently summarized in a study by Sugarman, et.al. (2018) [8].
Case presentation
A 50-year-old hypertensive female was admitted for recurrent dysarthria that had first occurred five days prior to admission lasting for two hours. At its onset, the patient did not experience other stroke-like symptoms, like aphasia, facial asymmetry, bulbar symptoms, hemiparesis, or hemianesthesia, but rather experienced light headedness, disorientation, and wrong responses to specific questions. She had been brought to the emergency department of another hospital, where her symptoms spontaneously resolved, and was advised to obtain a cranial MRI and MRA if her symptoms recurred. Ten hours prior to admission, her dysarthria and light headedness had recurred, lasting for ten minutes. She had a previous history, three months prior to admission, of a 10-day history of pericardial effusion, and dyspnea and had undergone pericardiocentesis. She also had a two-week history of episodic hematuria, thrombocytopenia, and a non-pruritic macular rash over her palms and soles 17 days prior to the current admission. None of these etiologies were disclosed to the patient. On neurological examination, she had an NIHSS score of zero, pallor with pale palmar creases, non-blanching non-pruritic macules over the fingertips, toes, and soles (Figure 1). An acute ischemic stroke in the cortical area from a small vessel occlusion versus a hypercoagulable nature was being entertained.
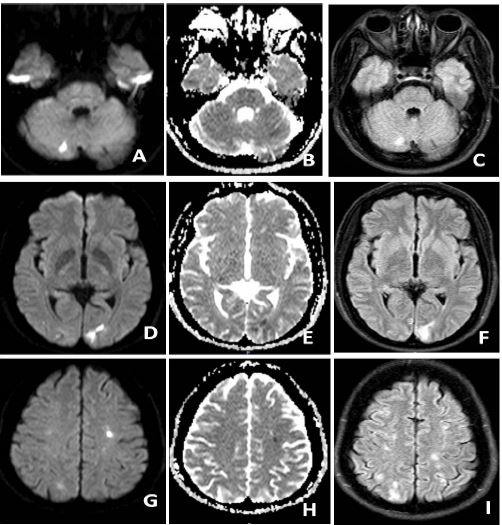
In the emergency room, she had remained awake and responsive with no signs of cardiorespiratory distress nor fainting. In transit to the NCCU, a plain cranial MRI/MRA revealed multiple acute infarcts in the bilateral frontal corona radiata, centrum semi-ovale, parieto-occipital lobes, and a chronic infarct in the right inferior cerebellum, and mildly atherosclerotic internal carotid arteries, while laboratory tests had shown findings suggestive of TTP, such as, normochromic normocytic anemia from hemolysis as confirmed by a positive Direct Coombs’ test, thrombocytopenia, elevated unconjugated bilirubin and lactate dehydrogenase levels, and peripheral blood smear findings of lysed erythrocytes and schistocytes (Figure 2, and Table 1). The PLASMIC score was computed at five, an intermediate score, ideally warranting the sample be tested for the plasma protease, ADAMTS-13 levels. Venous compression test done showed a chronic superficial venous thrombosis in the left saphenous vein.

Table 1: Complete blood count, electrolyte, LDH, and bilirubin level trends since admission.
| Parameter | Normal value | Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 6 | Day 7 |
|---|---|---|---|---|---|---|---|---|
| Hemoglobin | 11.6-15.5 g/dL | 7.0 | 6.7 | 5.4 | 7.6 | 7.9 | 11.7 | 11.6 |
| Hematocrit | 36-47% | 20.6 | 19.8 | 15.8 | 22.6 | 23.4 | 35.1 | 35.5 |
| WBC count | 4800-10800 mm3 | 5600 | 2800 | 8200 | 18600 | 15000 | 18600 | 9410 |
| Platelets | 150000-400000/ mm3 | 14000 | 21000 | 114000 | 169000 | 168000 | 246000 | 245000 |
| LDH | 120-246 U/L | 722 | 409 | |||||
| Total bilirubin | 0.3-1.2 mg/dL | 1.8 | 0.84 | |||||
| Conj bilirubin | 0 – 0.3 mg/dL | 0.48 | 0.26 | |||||
| Unconj bilirubin | 0 – 0.8 mg/dL | 1.32 | 0.58 |
At the NCCU, packed red blood cells and platelet pheresis were transfused. Tabulated in the first table are the relevant comparative laboratory parameters since admission until discharge. Eventually, TPE was started. Stroke guidelines in setting target parameters were followed, with a MAP set between 110 to 130 mmHg, and a positive fluid balance. With an index of suspicion for SLE, rheumatologic tests were also requested and completed on day four of admission revealing an SLEDAI score of 14 (positive for ANA1:320 with speckled pattern, serositis, hypocomplementemia; C3, Anti-smith, Anti-RNP, anemia, and thrombocytopenia). After two sessions of TPE, high dose steroids with MPPT intravenously for three days was given yielding substantial improvement in her clinical status. Her dysarthria did not recur, and repeat laboratory tests had shown a decrease in conjugated bilirubin and LDH, an increase in hemoglobin and platelet count, and the disappearance of the patient’s dermatologic condition. On the fifth hospital day, she was then started on Aspirin, Telmisartan/Amlodipine, and followed by Hydroxychloroquine on the seventh hospital day. Another day of observation after being transferred out of the NCCU showed no worsening of her clinical status, and she was eventually discharged after eight days.
Discussion/conclusion
Pertinent in this case report is the uniqueness of a patient with a TTP-SLE overlap presenting with multiple ischemic strokes instead of a usually documented large vessel occlusion [8]. This is further depicted in a Korean study, wherein the development of TTP in patients with SLE can lead to debilitating symptoms or even morbidity, qualifying the need for intensive and immediate therapy [3]. There have been case reports of patients with SLE eventually diagnosed with TTP after some diagnostic dilemma due to their overlapping symptoms, or even TTP as the first manifestation of SLE [8]. With previous findings of pericardial effusion two months prior to the current admission, and beginning non-pruritic, non-blanchable macules over the fingertips, toes, and soles, these evidences implicate that an autoimmune condition or hematological disorder may have gone unnoticed until the patient manifested with a stroke. The laboratory findings attributed to TTP during the first few days of admission increased the index of suspicion for the disease.Hallmark manifestations of TTP such as microangiopathic hemolytic anemia, and thrombocytopenia, were evident given the laboratory and ancillary procedures performed. Despite a PLASMIC score of five, a blood sample was no longer sent out for ADAMTS-13 testing due to financial constraints. Cranial imaging findings showing a chronic cerebrovascular disease in the right inferior cerebellum, and microvascular white matter ischemic changes, may suggest previous silent strokes, manifesting inconspicuously, increasing her predisposition for a symptomatic event prior to the emergency room consult. Because previous studies had established that TTP and LVOs lead to debilitating neurological symptoms, the authors were under the impression that the patient, who had non-debilitating symptoms at the emergency room, and an NIHSS score of 0, would present similarly, but further investigation revealed a patient with TTP-SLE overlap, presenting as multiple ischemic infarcts instead. All these are further supported by the article of Albo, et al. (2022) that recurrent multi-territory ischemic strokes may arise from the deficient ADAMTS-13 protein in TTP [2]. The pathophysiology for both TTP and SLE deals with an increase in small vessel vasculopathies, micro-emboli formation, and compromised blood flow. The endpoint of ischemia is further complicated by the natural explanation of TTP, the absence of ADAMTS-13 which further induces systemic platelet aggregation, microvascular thrombosis, and intravascular hemolysis from fibrin deposition and mechanical trauma. There are claims that discrete ADAMTS13 dysfunction may lead to widespread, but subclinical end-organ damage that becomes clinically noticeable only by its dramatic effects on the function of the nervous system [7].
The treatment of stroke has been well established by the American Stroke Association (ASA), as recognized by the American Association of Neurology (AAN). Neurological deficits can range from a subtle state of confusion or a non-specific symptom such as headache to those as debilitating as ataxia, seizures, or even coma. However, given that the mechanism of stroke is not the common large vessel atherosclerosis or small vessel occlusion, treatment is dictated by the identified cause. TPE significantly improves the outcome in patients with TTP, and those left untreated have an increased probability of mortality by as high as 90% [9]. Literature dictates that TPE followed by high-dose steroid therapy are beneficial to the patient, but given that the patient had a stroke thrombolysis was not done due to thrombocytopenia and it was deemed more harmful than beneficial [4,9]. Previous studies have shown that almost all patients diagnosed with TTP underwent TPE. The bictyopenia of the patient was treated with pRBC transfusions, and platelet pheresis with a favorable response and stabilization of hemoglobin, hematocrit, and platelet count levels. Likewise, as studies and guidelines have established before, the patient responded well to TPE, and MPPT.She was transferred out of the NCCU, and had remained stable prior to discharge with the following medications: Telmisartan/Amlodipine besilate 40 mg/5 mg tab one tab daily, Aspirin 80 mg/tab one tablet daily, Hydroxychloroquine 200 mg/tab one tablet daily, tapering doses of Prednisone for two weeks, and Atorvastatin 40 mg/tab 1 tablet every bedtime.
In conclusion, this paper shares a rare case of a documented 50-year old Filipino woman with TTP-SLE overlap and multiple ischemic strokes manifesting with dysarthria responsive to TPE and MPPT despite not having been tested for ADAMTS13, implying that clinical judgment still accounts for majority of most pertinent diagnostic tests, life-saving therapeutic actions, and efforts to return the patient to their pre-morbid condition.
Declarations
Limitations: The limitations of this study is that no sample was sent for further ADAMTS-13 testing.
Acknowledgements: The authors would like to thank the institution for sharing this case. The authors of this study equally shared in the management, and assessment of the patient, including the generation of this paper.
Conflict of interest: The authors listed in this study have no conflicts of interest to declare.
Source of funds: The time and effort put into this case report did not receive any grant from any funding agency be it from a private, commercial or public sector.
References
- Adams HP Jr, Bendixen BH, Kappelle LJ, Biller J, Love BB, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of ORG 10172 in Acute Stroke Treatment. Stroke. 1993; 24: 35-41.
- Albo Z, Mathew C, Catton R, Silver, Moonis M. Thrombotic thrombocytopenic purpura (ADAMTS13 [a Disintegrin and Metalloproteinase with a Thrombospondin Type 1 Motif, Member 13] Deficiency) as a cause of recurrent multiterritory ischemic strokes. Stroke, June 2022; 53: e237 – e 240.
- Kwok SK, Ju JH, Cho CS, Kim HY, Park SH, et al. Thrombotic thrombocytopenic purpura in systemic lupus erythematosus: risk factors and clinical outcome: A single centre study. Lupus. 2009.
- Knobl P. Thrombotic thrombocytopenic purpura. Magazine of European medical oncology. 2018; 11: 220-226.
- Nikolopoulos D, Fanouriakis A, andBoumpas DT. Cerebrovascular events in systemic lupus erythematosus: diagnosis and management. Mediterranean Journal of Rheumatology. 2019; 30: 7-15.
- Opeyemi FB, Akintayo RO, Bojuwoye MO, Alabi TO, Akintayo FC, et al. hrombotic thrombocytopenic purpura as the first presentation in systemic lupus erythematosus. Reumatologia. 2018; 56: 268-270.
- Rojas JC, Banerjee C, Bourbakhsh B, Powell CM. Pearls & Oy-sters: Acute ischemic stroke cause by atypical thrombotic thrombocytopenic purpura. American Academy of Neurology. 2013; 80: e235-e238.
- Sugarman R, Tufano AM, Liu JM. Large vessel stroke as initial presentation of thrombotic thrombocytopenic purpura. BMJ Case Reports. 2018.
- Yamada R, Nozawa K, YoshiminaT, Takasaki Y, Ogawa H, et al. A case of thrombotic thrombocytopenic purpura associated with systemic lupus erythematosus: Diagnostic utility of ADAMTS-13 activity. Autoimmune Diseases. 2011.
- Zheng XL, Vesely SK, Cataland SR, Coppo R, Geldziler B, et al. ISTH guidelines for treatment of thrombotic thrombocytopenic purpura. Journal of Thrombosis and Haemostasis. 2020; 18: 2496 – 2502.