
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Mastoid adenocarcinoma revealed by chronic otitis media
Myriam Loudghiri*; Hamza Benghaleb; Youssef Oukessou; Sami Rouadi; Redallah Abada; Mohamed Roubal; Mohamed Mahtar
Otorhinolaryngology and Head and Neck Surgery Department, IBN ROCHD University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
*Corresponding Author : Myriam Loudghiri
Otorhinolaryngology and Head and Neck Surgery Department, IBN ROCHD University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
Tel: +21 2665466153;
Email: m.loudghiri@hotmail.com
Received : Mar 05, 2023
Accepted : Mar 23, 2023
Published : Mar 30, 2023
Archived : www.jcimcr.org
Copyright : © Loudghiri M (2023).
Abstract
The diagnosis of primary carcinoma in the mastoid bone is usually made while performing a mastoidectomy in an effort to control presumed chronic mastoiditis. The chronic infection, purulent otorrhea, and severe otalgia, are the main warning signs of carcinoma of the middle ear or external auditory canal. If the amount of bony mastoid destruction is out of proportion, malignancy should be strongly suspected.
Keywords: Mastoid bone; Carcinoma; Chronic mastoiditis; Otalgia; Mastoidectomy.
Citation: Loudghiri M, Benghaleb H, Oukessou Y, Rouadi S, Abada R, et al. Mastoid adenocarcinoma revealed by chronic otitis media. J Clin Images Med Case Rep. 2023; 4(3): 2347.
Introduction
Malignant tumors of the mastoid and middle ear are rare. Squamous cell carcinoma being the most common malignancy in head and neck region, is also most common variety found in temporal bone tumors [1]. Other varieties are adenocarcinoma, adenocystic carcinoma, mucoepidermoid carcinoma, ceruminous carcinoma and rhabdomyosarcoma.
The incidence of primary temporal bone tumors ranges between 0.03-1.0 per 100000 per year and approximately 60-80% are squamous cell carcinoma [2].
The tumors of tympano-mastoid region are more common in elderly persons in 6th and 7th decade. Males are more commonly affected than females. Various predisposing factors have been proposed like chronic suppurative otitis media, prior exposure to radiations in nasopharyngeal, intracranial and head and neck cancers and ultraviolet radiations. The presentation of these tumors is usually like Chronic Suppurative Otitis Media (CSOM) which makes the diagnosis very difficult and even after diagnosis, treatment is very challenging and unrewarding with a very high recurrence and mortality rate.
Case report
An 81-year-old woman, with medical past history of arterial hypertension, was referred to our department for a 1 year right-side dotalgia, purulent otorrhea and important hearing loss. The patient had not experienced any other otologic symptoms.
Clinical examination revealed an obvious inflammation and stenosis of the right external auditory canal, with no facial palsy.
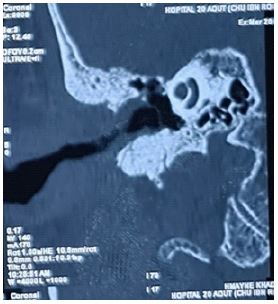
The CT scan showed a mucosal thickening of the different walls of the external auditory canal, along with lysis of the tympanal bone, and a blunted scutum, suspecting a malignant external otitis (Figures 1 and 2).
The patient has been admitted the first time and several further times for the same symptomatology, and was treated with intravenous large spectrum of antibiotics, antifungal drugs and local treatment with no significant amelioration.
A biopsy of the right external auditory canal was performed, the histological result was not conclusive.
With the non-amelioration, and the worsening of the pain, a diagnostic mastoidectomy has been performed, revealing in the histological study a poorly differentiated and invasive adenocarcinoma (CK7+ / CK20-).
Later on, an open mastoidectomy was performed, before referring the patient to oncology for further treatment.

Discussion
Tumors of temporal bone which includes malignancies of skin of pinna and external auditory canal, middle ear mastoid, petrous bone and metastatic lesions are very rare entity.
The incidence has been reported ranges between 0.03-1.0 per 100000 per year and it is more common in males in age group of 6th and 7th decade.
Many etiological factors have been reported like previous radiation exposure, ultraviolet radiation and chronic otitis media [1]. Chronically discharging ears are considered as risk factor in many studies which may be due to metaplasia in the middle ear mucosa due to chronic infection.
In our care report, the patient had long standing ear discharge for more than one year.
Some studies have also considered agents such as chlorinated disinfectants or human papillomavirus in cases of carcinomas associated with inverted papilloma as possible carcinogens [3-5].
The clinical features are very similar to chronic otitis mediarendering diagnosis very difficult. The most common symptoms are long standing blood-tinged ear discharge, severe pain, rapidly growing polypoidal or granulomatous mass in EAC or Middle Ear, peripheral facial palsy and painless ulceration over pinnaor EAC. A high index of suspicion in such cases should render a clinician for thorough clinical examination and investigation to rule out malignancy. Radiological investigations play a very important role in diagnosis in suspicious cases. CT scan for bony erosion and MRI for soft tissue involvement and neural invasion are investigations of choice. Tissue biopsy is must for histopathological examination and diagnosis.
Surgery and chemo-radiotherapy are the mainstay of treatment.
Chemotherapy can also be considered in cases with post-surgical residual disease or recurrence, distant metastasis and conditions where surgery and radiotherapy are contraindicated.
Conclusion
Temporal bone tumors are rare but very aggressive and difficult to treat.
Diagnosis becomes very difficult as the clinical features are most of the time similar to chronic suppurative otitis media.
Strong suspicion is required for timely diagnosis and treatment to improve survival.
References
- National Cancer Institute. “Cancer facts. Head and neck cancer: Questions and answers.” Available at: http://www.cancer.gov/cancertopics/factsheet/Sitestypes/head-and-neck/. Accessed on 3 February 2018.
- Lionello M, Stritoni P, Facciolo MC, Staffieri A, Martini A, et al. Temporal bone carcinoma. Current diag-nostic, the rapeutic, and prognostic concepts. J Surg Oncol. 2014; 110: 383- 392.
- Monem SA, Moffat DA, Frampton MC. Carcinoma of the ear: a case report of a possible association with chlorinated disinfectants. J Laryngol Otol. 1999; 113: 1004-1007.
- Gaio E, Marioni G, Blandamura S, Staffieri A. Inverted papiloma involving the temporal bone and its association with squamous cell carcinoma: critical analysis of the literature. Expert Rev Anticancer Ther. 2005; 5: 391-397.
- Marioni G, Altavilla G, Busatto G, Blandamura S, De Filippis C, et al. Detection of human papilloma virus in temporal bone inverted papilloma by polymerase chain reaction. Acta Otolaryngol. 2003; 123: 367-371.