
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Malignant ascites with irreducible pelvic organ prolapse
Rosemary Noel Senguttuvan; Shiva Hadadianpour*; Christopher P Chung
Department of Gynecologic Oncology, City of Hope Comprehensive Cancer Center, Duarte, CA, USA.
*Corresponding Author : Shiva Hadadianpour
Department of Gynecologic Oncology, City of Hope Comprehensive Cancer Center, Duarte, CA, USA.
Email: shivahadadian@yahoo.com
Received : Mar 10, 2023
Accepted : Mar 24, 2023
Published : Mar 31, 2023
Archived : www.jcimcr.org
Copyright : © Hadadianpour S (2023).
Citation: Senguttuvan RN, Hadadianpour S, Chung CP. Malignant ascites with irreducible pelvic organ prolapse. J Clin Images Med Case Rep. 2023; 4(3): 2350.
Description
Two women with gastrointestinal malignancies leading to increased abdominal pressure from their copious ascites presented with irreducible pelvic organ prolapse.
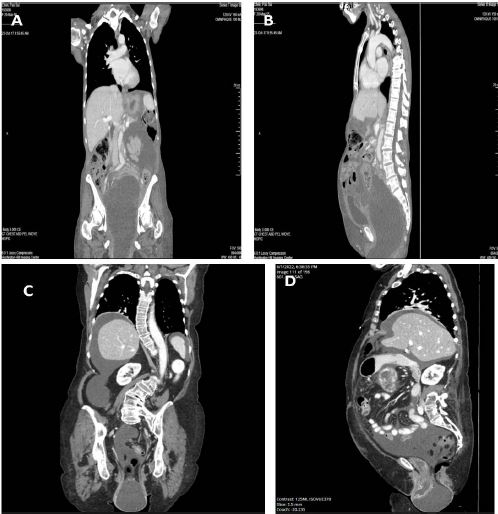
The first patient is a 62-year-old para 2 with a diagnosis of low-grade mucinous adenocarcinoma suspected to be arising from the appendix who was referred to urogynecology service for worsening pelvic organ prolapse. Radiographically, she had evidence of diffuse carcinomatosis with pseudomyxoma peritonei, and associated pelvic organ prolapse (Figure 1A and 1B). Physical examination showed stage IV uterovaginal prolapse. Pessary placement was attempted in office but failed due to irreducible nature of the prolapse. Due to the patient’s worsening disease course, she was transitioned onto hospice and her prolapse was expectantly managed.
The second patient is a 70-year-old para 3 with a history of prior hysterectomy who had irreducible stage IV vaginal vault prolapse secondary to her malignant ascites from her gastrointestinal stromal tumor primary. As evidenced by her radiographic images (Figure 1C and 1D), her prolapse extended to 10 cm past her hymenal ring. She underwent a joint surgical procedure for tumor debulking of her disease through midline laparotomy and with concurrent transvaginal anterior/posterior colporrhaphy, perineoplasty, and uterosacral ligament suspension. More than 2 liters of mucinous ascites was evacuated transvaginally.
Patients with ascites from gastrointestinal malignancy can have associated irreducible pelvic organ prolapse. These patients should be managed jointly with their oncologist, and joint surgery can be performed when indicated to improve their quality of life [1-3].
Declarations
Disclosure statement: The authors report no conflicts of interest.
Author contributions: Rosemary Noel Senguttuvan, MD: First author who selected images and wrote main text.
Shiva Hadadianpour, MD: Author who assisted with main text editing.
Christopher P. Chung, MD: Author who served as expert in the field and oversaw selection of patients, images, and was final editor of main text.
References
- Chung et al. Prolapse Repair After Anterior Exenteration. Int Urogynecol J. 2021; 32: 1037-1038.
- Kohut et al. Feasibility of combining pelvic reconstruction with gynecologic oncology-related surgery. Int Urogynecol J. 2023; 34: 177-183.
- Chung CP, Lee SJ, Wakabayashi MT. Chung CP, Lee SJ, et al. Am J Obstet Gynecol. 2018; 219: 621-622.